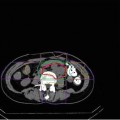
Fig. 26.1
Typical dose distribution for pancreatic cancer. The image is from a case of a 75-year-old man with cancer in the head of the pancreas that received 52.8 GyE/12 fr. It is possible to deliver a high dose to the tumor and neuroplexus whilst minimizing the dose to the surrounding organs such as the stomach or duodenum
26.3 The Pancreatic Cancer Trial at National Institute of Radiological Sciences
We started a phase I/II clinical trial for preoperative C-ion RT delivered in 16 fractions over 4 weeks for resectable pancreatic cancer in 2000 (Fig. 26.2).
Fig. 26.2
The clinical trial pathway for C-ion RT in pancreatic cancer
The purpose of this treatment was to reduce the risk of postoperative local recurrence, which accounts for approximately 50 % of all recurrences. We established the tolerance and effectiveness of preoperative C-ion RT and performed an additional clinical trial aimed at reducing the number of fractions to 8, delivered over 2 weeks beginning in 2003 (protocol 0203). In addition, we started a phase I/II clinical trial for patients with locally advanced pancreatic cancer and showed that the treatment was safe and provided excellent local control rates. As a result, we are currently performing a clinical trial using C-ion RT combined with gemcitabine (protocol 0513).
26.4 Carbon Ion Radiotherapy Methodology at National Institute of Radiological Sciences
The key features of the accelerator and the carbon ion beam have been described previously [11].
26.4.1 Patient Immobilization
The patient needs to be immobilized during C-ion RT for pancreatic cancer as is the case for other tumor sites. C-ion RT at facilities with the most powerful heavy-ion beams is performed with fixed beam directions that are vertical, horizontal, or at a 45-degree oblique angle to the target. However, recurrent rectal tumors can be located anywhere in the pelvis, including the presacral region and iliac and mesenteric lymph nodes, and therefore, the direction of the carbon ion beam needs to be varied. Furthermore, it is usually necessary to use more than two ports in order to obtain a dose distribution that avoids the bowels and the skin. Consequently, complex immobilization is frequently required.
At the National Institute of Radiological Sciences (NIRS), this was achieved using relatively thick, low-temperature thermoplastic (Shellfitter; Keraray Co., Ltd., Osaka, Japan), a sufficiently large customized cradle (Moldcare; Alcare, Tokyo, Japan), and a rotatable couch on the treatment bed.
Management of respiratory motion is also essential in most cases of recurrent rectal cancer (see Chap. 9, Motion Management). There are many different methods for motion management. At the NIRS, synchronization with respiration is adopted during both computed tomography (CT) image acquisition and during every C-ion RT session, irrespective of the direction of the beam. The effect of respiratory motion when using a vertical beam is less than that when using a horizontal beam for a pelvic tumor. However, this is mainly due to differences in the length of the air gap, and it is desirable to irradiate the tumor using similar conditions to those established by dose calculations using CT images taken during the expiratory phase.
26.4.2 Target Delineation
A set of 2.5-mm-thick CT images along the whole abdomen were taken for treatment planning, with the patient placed in immobilizing devices and with respiratory gating.
Field arrangements were generally designed using a 3- or 4-field plan. The gross tumor volume (GTV) was established using CT images and margins for possible subclinical tumor spread, and magnetic resonance imaging (MRI) and fludeoxyglucose (FDG)-positron emission tomography were used to diagnose tumor spread. The clinical target volume (CTV) was defined as the gross volume plus 0.5 or 0 cm (in contact with the duodenum or stomach). The CTV included the GTV, neuroplexus, and regional lymph nodes. The latter consisted of the celiac, superior mesenteric, common hepatic, and peri-pancreatic lymph nodes (Fig. 26.1). At least 50 % of the functioning renal parenchyma received a dose of 15 GyE or less, and the spinal cord dose was limited to 30 GyE or less. Planning target volume (PTV) is defined as the CTV with a margin of at least 5 mm in all directions, although these margins are modified if critical organs, such as the skin or bowels, are close to the tumor.
26.4.3 Dose Prescription
The current recommended dose is 55.2 GyE delivered in 12 fractions for locally advanced pancreatic cancer and 35.2 GyE delivered in 8 factions for resectable pancreatic cancer. The whole of the prescribed dose is given at the maximum dose point of each portal, and treatment planning is performed so that the PTV is covered with at least 90 % of the prescribed dose. For this purpose, additional margins are necessary to determine the shape of the collimator and compensation bolus. Figure 26.1 shows a representative dose distribution for C-ion RT as it is currently used at the NIRS.
Major organs at risk during this treatment are the stomach, duodenum, intestine, kidney, and spinal cord. It is particularly important to spare the bowels from the high-dose area of the carbon ion beam. At the NIRS, dose constraints for the digestive tract are established on the basis of the treatment results for prostate, uterine, cervical, and recurrent rectal cancers, where the maximum dose to the colon should not exceed 83 % of the prescribed dose.
26.4.4 Field Positioning and Irradiation at National Institute of Radiological Sciences
At the NIRS, C-ion RT is performed once a day and in 4 fractions per week (from Tuesday until Friday). The field is verified at every treatment session using a computer-aided online positioning system to prevent the positioning error exceeding 2 mm. A fluoroscopic image is taken during the expiration phase of respiration and compared with the reference images, including the image taken during the previous simulation or the digitally constructed radiograph. C-ion RT is performed with respiration gating as described above, where the carbon ion beam is delivered only during the expiration phase.
26.5 Results of Carbon Ion Radiotherapy Used at the National Institute of Radiological Sciences
26.5.1 Preoperative Carbon Ion Radiotherapy for Patients with Resectable Pancreatic Cancer
The purpose of this study was to evaluate the safety and efficacy of C-ion RT as preoperative treatment and to determine the optimum dose needed to reduce the risk of postoperative local recurrence without causing unacceptable damage to normal tissue.
The eligibility criteria for this study were that the pancreatic cancer was judged radically resectable and that it did not involve the celiac trunk or superior mesenteric artery. We performed C-ion RT with 8 fractions over 2 weeks, followed by resection 2–4 weeks later (Fig. 26.2). The first dose was 30 GyE over 8 fractions, and this was then increased in 5 % increments.
Twenty-six patients were enrolled between April 2003 and December 2010, and the initial dose of 30 GyE was ultimately escalated to 36.8 GyE.
We administered C-ion RT to all patients as scheduled. The clinical stage according to the UICC was IIA in 15 cases and IIB in 11 cases. Twenty-one out of 26 patients received curative resection (resection rate 81 %), although the remaining five patients did not undergo surgery due to liver metastases or refusal of treatment. Although grade 3/4 toxicities were noted in 2 patients (liver abscess in one and PV thrombus in the other), neither were directly related to C-ion RT. No other serious adverse effects were observed. In the 21 surgical cases, the 5-year local control and overall survival rates were 100 and 52 %, respectively (Fig. 26.3). In the literature, the reported 5-year survival rates for pancreatic cancer treated with resection were 20–30 % (Table 26.1).
Fig. 26.3
Local control and overall survival. The local control rate in all patients was 100 %. There were no cases of recurrence within the irradiated lesion. The 5-year OS rate among patients who underwent resection was 55 %
Table 26.1
Results of preoperative chemoradiotherapy
Year | n | Treatment |
|---|