CHAPTER 24 Paraganglioma
Epidemiology
Temporal bone paragangliomas/chemodectomas are most commonly found along cranial nerves IX and X. Within the temporal bone region, they occur in the middle ear cleft on the cochlear promontory (20%) or the hypotympanum (25%) as glomus tympanicum tumors, the jugular foramen region (50%) as glomus jugulare tumors, or just below the skull base (5%) as glomus vagale tumors. Lesions involving the middle ear and jugular fossa regions are called glomus jugulotympanicum tumors. Paragangliomas are the most common primary middle ear neoplasm.
The incidence of temporal bone paragangliomas is approximately 1/million/year, and somewhat preferentially occur in middle-aged women.
When spontaneously occurring, these lesions are multiple in 5 to 10% of patients, but are multiple in up to 50% of patients in familial cases.
Clinical Features
Presenting symptoms in patients with these neoplasm are a function of the location of the tumor. Middle ear lesions (glomus tympanicum tumors) can present with pulsatile tinnitus (80 to 90%) as theyare vascular tumors, conductive hearing loss (50 to 60%) as ossicles can be affected, otalgia, or simplya sense of ear “fullness.” Less than 5% of these tumors are physiologically active, producing catecholamines (norepinephrine). Middle ear paragangliomas are essentially never physiologically active. On physical examination, these lesions can be seen as a reddish vascular mass behind the anteroinferior portion of the tympanic membrane.
Pathology
All paragangliomas/chemodectomas, regardless of location, are histologically identical. They arise from embryonic neural crest cells that have differentiated into paraganglia (chemoreceptor cells). These extremely vascular, but histologically benign tumors are composed of central “chief” cells that are arranged in a typical pattern called “zellballen.” Less than 5% of these “chief” cells actively secrete catecholamines. More aggressive tumor variants can have similar histology but can only be diagnosed when metastatic lesions are present (<5% of patients).
Treatment
Preoperative endovascular embolization, surgery, or radiation therapy are potential therapies for larger lesions. Smaller lesions (which include essentially all lesions confined to the middle ear region) are usually treated with surgery only. Complete resection is curative.
Imaging Findings
When tumors are large, their respective site of origin can be obscure, as the jugular foramen, middle ear, and petrous temporal bone regions may all be involved. Such large tumors of the temporal bone may simply be referred to as glomus jugulotympanicum tumors and should be characterized with computed tomography (CT) (osseous involvement) and magnetic resonance imaging (MRI) (intracranial and infratemporal extension; differentiating tumor from trapped middle ear or mastoid secretions). When confined to the middle ear cleft, these tumors can arise anywhere on the medial wall of the mesotympanum and hypotympanum (i.e., along the course of the tympanic branch of cranial nerve IX), not just the cochlear promontory region, and are considered glomus tympanicum tumors. Such smaller tumors can be adequately characterized with CT without the need for MRI.
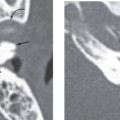
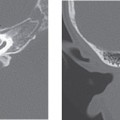
CT
High-resolution (1 to 2 mm) noncontrast CT performed in the axial and coronal planes and reconstructed with a detail (bone) algorithm best delineates temporal bone structures. Sagittal reformatted images may also prove useful.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


