Parameniscal Cyst
KEY FACTS
Imaging
IMAGING
General Features
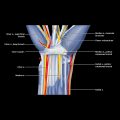
 Extension from parameniscal area on medial and lateral aspects of knee
Extension from parameniscal area on medial and lateral aspects of knee
 Cysts from medial meniscus often extend either
Cysts from medial meniscus often extend either
 Cysts from lateral meniscus often extend deep to iliotibial tract or lateral collateral ligament
Cysts from lateral meniscus often extend deep to iliotibial tract or lateral collateral ligament
 Medial parameniscal cysts in particular can extend quite a distance from meniscal tear
Medial parameniscal cysts in particular can extend quite a distance from meniscal tear
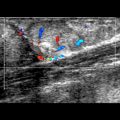
Ultrasonographic Findings
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Parameniscal Cyst










 on the medial aspect of the knee around the medial joint line due to a parameniscal cyst.
on the medial aspect of the knee around the medial joint line due to a parameniscal cyst.
 located superficial to the medial collateral ligament
located superficial to the medial collateral ligament  . The cyst is extending proximally
. The cyst is extending proximally  toward the knee joint.
toward the knee joint.
 extending through the medial collateral ligament
extending through the medial collateral ligament  toward the periphery of the thinned degenerate medial meniscus
toward the periphery of the thinned degenerate medial meniscus  .
.
 , with meniscal mucoid degeneration
, with meniscal mucoid degeneration  and a small parameniscal cyst
and a small parameniscal cyst  arising from the peripheral aspect of the tear. Meniscal tears are much better depicted on MR than US.
arising from the peripheral aspect of the tear. Meniscal tears are much better depicted on MR than US.