Part 3 Gastrointestinal Tract
Case 70

Key Finding
Irregular distal esophageal mucosa with stricturing.
Top 3 Differential Diagnoses
Esophageal carcinoma: Squamous cell carcinoma (SCC) is the most common carcinoma and typically occurs in the upper and midesophagus while adenocarcinoma typically occurs distally. For SCC, the most common risk factors are smoking and alcohol while adenocarcinoma arises from Barrett’s esophagus due to chronic reflux. Most appear as an irregular mass causing stricture with ulceration and shouldered edges. Superficial carcinomas can also have a plaque-like, polypoid, or ulcerative appearance. A rare varicoid type can appear similar to esophageal varices, but does not change with peristalsis.
Metastasis: The esophagus is most commonly involved by direct invasion, hematogenous metastases are rare. Lung and breast primaries typically involve the midesophagus through mediastinal lymph node metastases while gastric primaries directly invade the lower esophagus. The esophagus is the least common gastrointestinal location for lymphoma. Imaging features overlap with primary esophageal carcinoma. y Benign esophageal neoplasms: Represent approximately one-fourth of esophageal neoplasms and are typically asymptomatic. Leiomyoma is the most common mesenchymal tumor while gastric gastrointestinal stromal tumors (GISTs) predominate in the rest of the gastrointestinal tract. Additional benign tumors include adenomas, polyps, and foregut duplication cysts. Imaging findings are typically a smooth intramural or intraluminal mass without ulceration or nodularity.
Additional Diagnostic Considerations
Foreign body: History is often diagnostic except in children or the mentally impaired. Radiopaque foreign bodies are easily diagnosed with plain film. Large food boluses may appear as an irregular polypoid mass on barium examination. On resolution, the patient should be evaluated for underlying stricture or motility disorder.
Radiation esophagitis: Barium examination demonstrates a long smooth narrow stricture with small shallow ulcers and granular mucosa that can mimic a circumferential mass. The location should correspond to a known radiation port. Strictures develop approximately 4 to 8 months following a radiation dose of at least 50 Gy.
Diagnosis
Esophageal carcinoma.
✓ Pearls
Irregular esophageal stricturing is concerning for esophageal carcinoma.
Metastatic involvement of the esophagus is almost always through direct extension.
Benign tumors should have smooth margins.
Suggested Readings
Collazzo LA, Levine MS, Rubesin SE, Laufer I. Acute radiation esophagitis: radiographic findings. AJR Am J Roentgenol. 1997; 169(4):1067–1070 Gupta S, Levine MS, Rubesin SE, Katzka DA, Laufer I. Usefulness of barium studies for differentiating benign and malignant strictures of the esophagus. AJR Am J Roentgenol. 2003; 180(3):737–744 Lewis RB, Mehrotra AK, Rodriguez P, Levine MS. From the radiologic pathology archives: esophageal neoplasms: radiologic-pathologic correlation. Radiographics. 2013; 33(4):1083–1108Case 71

Key Finding
Left upper quadrant fat stranding.
Top 3 Differential Diagnoses
Acute pancreatitis: Most commonly caused by alcohol abuse or gallstones. Patients present with epigastric pain radiating to the back. There are two main subtypes, interstitial edematous and necrotizing. Interstitial edematous pancreatitis represents the majority of cases and demonstrates loss of the normal fatty lobulated contour with peripancreatic fat stranding. Necrotizing pancreatitis demonstrates areas of parenchymal necrosis, which will be nonenhancing and poorly circumscribed, along with a greater degree of peripancreatic fat stranding.
Diverticulitis: Diverticular disease most commonly affects the sigmoid colon. CT is used for evaluation of acute diverticulitis. Findings include segmental wall thickening and adjacent pericolonic inflammatory changes. Complications include perforation with pneumoperitoneum, abscess, and fistula formation. On CT, colonic wall thickening and pericolonic fat stranding are centered on the inflamed diverticulum.
Perforated gastric ulcer/gastritis: Gastritis can be associated with ulcers; the majority (95%) is benign in etiology. Associations include epigastric pain, nonsteroidal anti-inflammatory drug (NSAID) use, and H. pylori infection. On CT, findings include epigastric fat stranding, gastric wall thickening, and free intraperitoneal air (when perforated).
Additional Diagnostic Considerations
Abscess: On CT, findings include loculated, low-density fluid collection with peripheral rim enhancement, increased incidence in immunocompromised, diabetics, and postoperative patients. Prior to full abscess formation, phlegmon appears more like focal fat stranding without a discrete fluid collection.
Omental Infarct: A portion of the omental fat is infarcted secondary to arterial insult. The most common location is in the right lower quadrant. Patients present with acute right lower quadrant pain, fever, and a palpable mass. On CT, findings include focal fat stranding. Treatment is conservative and centers on pain management.
Diagnosis
Gastritis secondary to peptic ulcer disease.
✓ Pearls
Gastritis typically needs further evaluation with a barium fluoroscopy study.
Pancreatitis is a clinical diagnosis and CT only serves to exclude its sequelae.
When fat stranding is centered in the fat and not an organ consider omental infarct.
Suggested Readings
Federle MP, Jeffrey RB, Woodward PJ, Borhani A. Diagnostic Imaging: Abdomen. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009 Pereira JM, Sirlin CB, Pinto PS, Jeffrey RB, Stella DL, Casola G. Disproportionate fat stranding: a helpful CT sign in patients with acute abdominal pain. Radiographics. 2004; 24(3):703–715 Thornton E, Mendiratta-Lala M, Siewert B, Eisenberg RL. Patterns of fat stranding. AJR Am J Roentgenol. 2011; 197(1):W1:W14Case 72

Key Finding
Diffuse stomach wall thickening with luminal narrowing (linitis plastica).
Top 3 Differential Diagnoses
Gastric adenocarcinoma: Gastric adenocarcinoma is the most common malignancy of the stomach ( 90%). When it infiltrates the muscular layer of the stomach it results in muscular dysfunction. This muscular infiltration prevents normal gastric distention and results in narrowing of the lumen. This nondistensibility has been described as a “leather bottle” appearance (linitis plastica). Scirrhous carcinoma (disseminated) accounts for 5 to 15% of cases and usually begins in the pylorus and extends superiorly. Gastric carcinoma risk factors include nitrites, salted, and smoked foods. On CT, there is diffuse thickening of the stomach with disappearance of the rugal folds and a small lumen. Linitis plastica is indicative of advanced disease.
Metastasis: Metastatic disease to the stomach is relatively rare and only seen in 2% of cancer patients. It typically is a sign of stage IV disease with poor prognosis. The most common primary carcinoma that leads to gastric metastases is breast carcinoma. Breast metastasis can present as multiple small lesions or linitis plastica (leather bottle) appearance. Hematogenous spread of metastasis is the most common route for metastatic spread to the stomach. The most common carcinomas to spread hematogenously to the stomach are malignant melanoma, lung, and breast cancer.
Lymphoma: Lymphoma is the second most common malignancy of the stomach. Gastrointestinal lymphoma is most commonly seen in the stomach. Most commonly it is non-Hodgkin’s B-cell lymphoma (diffuse large B-cell lymphoma [DLBCL] and extranodal marginal zone C-cell previously MALT [mucosa associated lymphoid tissue]). Significant abdominal adenopathy may also be seen with lymphoma. Menetrier’s disease can mimic lymphoma of the stomach due to rugal fold thickening.
Additional Diagnostic Considerations
Sarcoid: Involvement of the gastrointestinal tract is rare but when it occurs it most commonly involves the stomach. Signs of sarcoid involvement are nonspecific and include mucosal or wall thickening or gastric ulcers. Gastrointestinal manifestations of sarcoid are usually associated with pulmonary disease.
Diagnosis
Gastric adenocarcinoma.
✓ Pearls
Gastric adenocarcinoma, lymphoma, and metastasis can all appear similar.
Linitis plastic tends to cause loss of rugal folds whereas lymphoma, Menetrier’s disease, and inflammatory processes of the stomach tend to accentuate them.
Gastric mass or wall thickening with significant adenopathy is considered to be lymphoma.
Suggested Readings
Federle MP, Jeffrey RB, Woodward PJ, Borhani A. Diagnostic Imaging: Abdomen. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009 Lewis RB, Mehrotra AK, Rodríguez P, Manning MA, Levine MS. From the radiologic pathology archives: gastrointestinal lymphoma: radiologic and pathologic findings. Radiographics. 2014; 34(7):1934–1953 Whitty LA, Crawford DL, Woodland JH, Patel JC, Nattier B, Thomas CR, Jr. Metastatic breast cancer presenting as linitis plastica of the stomach. Gastric Cancer. 2005; 8(3):193–197Case 73

Key Finding
Right lower quadrant fat stranding.
Top 3 Differential Diagnoses
Inflammatory disease: Crohn’s disease is an idiopathic condition leading to transmural bowel wall inflammation. Crohn’s disease may involve any portion of the gastrointestinal tract from the esophagus to the anus (most commonly involves the terminal ileum) and will demonstrate “skip lesions.” In contrast, ulcerative colitis inflammation is limited to the mucosa and it has continuous involvement from the rectum. Imaging features of Crohn’s disease include mucosal ulcerations (cobblestone appearance), fibrofatty proliferation (creeping fat), thickened/edematous folds, bowel wall enhancement, mesenteric fatty proliferation (comb sign), and submucosal thickening with fat/edema (fat halo sign/target sign).
Appendicitis: Acute appendicitis is inflammation of the appendix and is one of the most common reasons for abdominal surgery in young patients. It occurs after obstruction of the appendiceal lumen (appendicoliths account for one-third of cases) leading to transmural inflammation and eventually infarction or perforation. One of the main complications is abscess formation. The most specific CT finding is a dilated appendix (> 6 mm) with peripheral fat stranding. Additional findings include thickened appendiceal wall and hyperemia.
Infectious colitis: Infectious colitis is typically long segment. The causative agents include parasites, protozoa, bacteria, and viruses. There are variable imaging features including low attenuating bowel wall thickening, fat stranding, and multiple air-fluid levels from increased fluid/liquid feces. The accordion sign refers to oral contrast between extremely thickened colonic haustra.
Additional Diagnostic Considerations
Diverticulitis: Diverticular occlusion can occur in any part of the bowel but is most common distally. The diverticular inflammation may lead to erosion and potentially microperforation. On CT, fat stranding is seen adjacent to a high-density diverticulum. Complications include abscess and fistula.
Omental infarct: Infarction of the greater omentum is a rare cause of abdominal pain and is a result of omental torsion or venous thrombosis/insufficiency. It can be spontaneous; however, predisposing factors are obesity, congestive heart failure, recent abdominal surgery/trauma, or strenuous activity. The omentum infarcts less often than the small bowel or colon because of its rich gastroepiploic collateral vessel supply. Imaging features include a nonenhancing omental fatty mass.
Diagnosis
Diverticulitis of right colon.
✓ Pearls
Diverticulitis has focal fat stranding surrounding a diverticulum.
Identifying the ileocecal valve first on CT will sometimes help finding the appendix.
Crohn’s disease most commonly involves the terminal ileum and is characterized by skip lesions.
Suggested Readings
Choi SH, Han JK, Kim SH, et al. Intussusception in adults: from stomach to rectum. AJR Am J Roentgenol. 2004; 183(3):691–698 Pereira JM, Sirlin CB, Pinto PS, Jeffrey RB, Stella DL, Casola G. Disproportionate fat stranding: a helpful CT sign in patients with acute abdominal pain. Radiographics. 2004; 24(3):703–715 Thornton E, Mendiratta-Lala M, Siewert B, Eisenberg RL. Patterns of fat stranding. AJR Am J Roentgenol. 2011; 197(1):W1–14Case 74

Key Finding
Symmetric cecal wall thickening.
Top 3 Differential Diagnoses
Inflammatory Bowel disease: Idiopathic inflammatory diseases of the colon include both Crohn’s disease and ulcerative colitis. Common presenting symptoms are abdominal pain and diarrhea, with or without blood. Crohn’s disease can occur anywhere along the gastrointestinal tract, but most commonly involves the terminal ileum and proximal large bowel. Ulcerative colitis tends to involve the distal colon, but can involve the proximal colon with “backwash” ileitis, symmetric wall thickening either short or long segment, mesenteric lymphadenopathy, and peripheral fat stranding in active disease. Complications of Crohn’s disease include strictures, abscess, fistula, and sinus tract formation. Complications of ulcerative colitis include stricture and toxic megacolon. Chronic ulcerative colitis can lead to loss of haustra resulting in the classic “lead pipe” colon.
Adenocarcinoma: Colon cancer is one of the most commonly diagnosed cancers and is potentially curable if detected early. Approximately one-fourth of colon cancers occur in the cecum. Early cancers are often found on endoscopy; however, barium enema can show plaque-like or pedunculated polyps. On CT, asymmetric bowel wall thickening with luminal narrowing can be seen. Additional findings of pericolonic fat stranding and loss of the fat planes between colon and adjacent structures suggests local tumor extension. PET–CT is also used for staging, which is necessary to determine ideal patient management.
Typhlitis: Also known as neutropenic colitis, typhlitis is a necrotizing enterocolitis that occurs in neutropenic patients, most commonly those receiving chemotherapy for leukemia. Patients present with abdominal pain, bloody diarrhea, and right lower quadrant pain. The diagnostic study of choice is CT, which will show massive symmetric/circumferential wall thickening with mucosal edema (hypoattenuation) involving the cecum (may also involve the proximal colon and terminal ileum) and adjacent inflammatory stranding. In severe cases, bowel wall necrosis and perforation can occur.
Additional Diagnostic Considerations
Infectious Colitis: Bowel wall inflammation due to bacterial, viral, fungal, or parasitic infection. Yersinia, cytomegalovirus (CMV), Salmonella, tuberculosis, histoplasma, and ameba infections commonly involve the cecum and proximal colon. Pan colon involvement is typically seen with CMV and Clostridium.
Appendicitis: Acute appendicitis is a common cause of abdominal pain necessitating surgical intervention. Inflammation from acute appendicitis can spread to the cecum resulting in cecal wall thickening. Additionally, wall thickening can occur between the cecal lumen and base of the appendix.
Diagnosis
Neutropenic colitis, typhlitis.
✓ Pearls
Crohn’s disease is most commonly seen in the terminal ileum and proximal large bowel.
One-fourth of colon cancers occur in the cecum.
Typhlitis is seen in neutropenic patients commonly involving the cecum.
Suggested Readings
Boyd SK, Cameron-Morrison JD, Hobson JJ, et al. CT imaging of large bowel wall thickening. J Am Osteopath Coll Radiol. 2016; 5(2):14–22 Fernandes T, Oliveira MI, Castro R, Araújo B, Viamonte B, Cunha R. Bowel wall thickening at CT: simplifying the diagnosis. Insights Imaging. 2014; 5(2):195–208 Iyer RB, Silverman PM, DuBrow RA, Charnsangavej C. Imaging in the diagnosis, staging, and follow-up of colorectal cancer. AJR Am J Roentgenol. 2002; 179(1):3–13Case 75

Key Finding
Small bowel air-fluid levels.
Top 3 Differential Diagnoses
Mechanical obstruction: Most classic association with air-fluid levels as noted on an upright radiograph. Typically, mechanical obstruction is associated with differential air-fluid levels, meaning levels are seen “stacked” or at different levels when viewed on the frontal upright abdominal film. The positive predictive value of differential air-fluid levels in small bowel obstruction is highest at levels of 20 mm or greater in height. This is seen in conjunction with dilated small bowel loops that are greater than 2.5 cm in diameter when measuring from outer wall to outer wall. The most common causes are overwhelmingly postsurgical adhesions (developed world) and hernias (developing world).
Ileus: A term used to describe aperistaltic bowel not caused by mechanical obstruction. It typically presents with non-colicky abdominal pain that is prolonged and often occurs after surgery. Radiographically it can be difficult to distinguish from mechanical obstruction as many features overlap. In contrast to mechanical obstruction, air-fluid levels are seen at the same level as opposed to “differential” as seen in mechanical obstruction. CT will also demonstrate lack of a transition point and lack of distal decompressed loops of small and large bowel. Medications have also been implicated, most commonly opioids.
Sentinel loop: Sentinel loop refers to a localized dilated loop of small bowel which is adjacent to a site of intra-abdominal inflammation. The sentinel loop often has an associated air-fluid level. This is not diagnostic of an intra-abdominal process but is an associated feature. Therefore, the sentinel loop prompts further evaluation with cross-sectional imaging when seen on abdominal imaging.
Additional Diagnostic Considerations
Inflammation: A few air-fluid levels within nondilated loops of small bowel are usually not clinically significant. Occasionally, this can be seen in a patient with underlying inflammatory gastroenteritis.
Diagnosis
Postoperative ileus.
✓ Pearls
Differential air-fluid levels are commonly associated with mechanical small bowel obstruction.
Air-fluid levels seen at the same level on an upright X-ray are likely due to ileus.
Sentinel loop refers to a dilated loop of small bowel containing air-fluid level adjacent to an inflammatory process.
Suggested Readings
Federle MP, Jeffrey RB, Woodward PJ, Borhani A. Diagnostic Imaging: Abdomen. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009 Harlow CL, Stears RL, Zeligman BE, Archer PG. Diagnosis of bowel obstruction on plain abdominal radiographs: significance of air-fluid levels at different heights in the same loop of bowel. AJR Am J Roentgenol. 1993; 161(2):291–295 Silva AC, Pimenta M, Guimarães LS. Small bowel obstruction: what to look for. Radiographics. 2009; 29(2):423–439Case 76

Key Finding
Perirectal cyst.
Top 3 Differential Diagnoses
Abscess: Perirectal abscess is an infected collection in perirectal region often associated with a perianal fistula. These occur most commonly spontaneously secondary to impaired drainage of the anal glands. Approximately 10% of cases are related to pelvic infections, trauma, cancer, inflammatory bowel disease, and radiation therapy. On CT, the classic findings include ring enhancing, fluid attenuated focus with peripheral fat standing. Greater than 80% of patients will develop a fistula chronically. Antibiotic therapy may result in spontaneous resolution while some require surgical reduction.
Duplication cyst: Perirectal cysts are rare congenital lesions from embryonic hindgut. They are also known as tailgut duplication cyst or retrorectal cystic hamartomas. They have a strong female predilection and are often asymptomatic. These cysts are typically posterior to the rectum. Complications include infection and bleeding. Malignant degeneration has been reported. Surgical excision is preferred treatment.
Inflammatory bowel disease: Crohn’s disease and ulcerative colitis may both affect the rectum. Crohn’s disease currently affects half a million people in North America. Crohn’s disease patients typically present in the third decade of life with bloody diarrhea, frequent small bowel movements, abdominal pain, and tenesmus. Imaging is optimally performed with CT or MRI enterography technique that is superior to barium fluoroscopy. Crohn’s disease more commonly involves the right colon but can involve any portion of the gastrointestinal tract. Crohn’s disease is associated with discontinuous transmural ulceration, which can develop both perirectal abscess and fistula formation. Fistula formation can occur between bowel loops, vagina, urinary bladder or abdominal wall/skin.
Additional Diagnostic Considerations
Lymphogranuloma venereum: Lymphogranuloma venereum is a sexually transmitted disease caused by Chlamydia trachomatis and may result in proctitis and or colitis. It is more common in men and is a granulomatous inflammatory response to the infected mucosa. Rectal involvement is common. Lymphogranuloma venereum may lead to perirectal abscess and fistula formation. Tetracycline is used for acute treatment.
Diagnosis
Spontaneous perirectal abscess.
✓ Pearls
The majority of perirectal abscesses occur spontaneous due to impaired drainage of the anal glands.
A retrorectal cyst without inflammatory changes should be considered a duplication cyst.
When an abscess is seen carefully evaluate for a fistula.
Suggested Readings
Boyd SK, Cameron-Morrison JD, Hobson JJ, Saenz R. CT imaging of large bowel wall thickening. J Am Osteopath Coll Radiol. 2016; 5(2):14–22 Hayelar M, Griepentrog K. Tailgut cyst: case report and literature review. Int J. Surg Case Rep. 2015; 10:166–168 Khati NJ, Sondel Lewis N, Frazier AA, Obias V, Zeman RK, Hill MC. CT of acute perianal abscesses and infected fistulae: a pictorial essay. Emerg Radiol. 2015; 22(3):329–335 O’Malley RB, Al-Hawary MM, Kaza RK, Wasnik AP, Liu PS, Hussain HK. Rectal imaging: part 2, perianal fistula evaluation on pelvic MRI—what the radiologist needs to know. AJR Am J Roentgenol. 2012; 199(1):W43:W53Case 77

Key Finding
Outpouching of the distal esophagus above the diaphragm.
Top 3 Differential Diagnoses
Epiphrenic pulsion diverticulum: Pulsion diverticula typically arise from the right posterior–lateral esophageal wall. These are not “true” diverticula as they are result of mucosal layer herniating through muscular layer. Diverticula are best seen on barium esophagram and appear as a focal luminal outpouching. The diverticula are a result of increased intraluminal pressure causing protrusion of the mucosa through the muscular wall. These are strongly associated with esophageal dysmotility. Epiphrenic diverticulum may present as a retrocardiac mass on a frontal chest X-ray and in this scenario are difficult to distinguish from a hiatal hernia.
Hiatal hernia: Herniation of abdominal contents through the esophageal hiatus. The majority involve superior displacement of gastroesophageal junction above the hiatus (sliding type). There may also be superior herniation of the gastric fundus which may present as left-sided retrocardiac mass with air-fluid level on chest X-ray. Less commonly the gastroesophageal junction may remain in normal position while the stomach herniates superiorly through the hiatus (paraesophageal type). Hiatal hernias will be seen on barium studies as a pouch above the diaphragm containing gastric rugae.
Prominent phrenic ampulla: Also known as the esophageal vestibule, it is the portion of the esophagus lying between the A and B rings. The phrenic ampulla is a normal structure that may be more prominent in some patients. Distinguishable from other entities on barium studies due to the normal position of the lower esophageal sphincter and its lack of gastric rugae.
Additional Diagnostic Considerations
Eosinophilic esophagitis: Inflammation of the esophagus with characteristic infiltration of eosinophils. Most characteristic imaging finding is concentric esophageal strictures on barium swallow (ring esophagus). It can be seen anywhere along the gastrointestinal tract and may manifest as fold thickening and submucosal edema within the bowel. Most of those affected have allergy/food intolerance history. Biopsy of esophagus is required for definitive diagnosis. Eosinophilic esophagitis responds well to steroid treatment.
Diagnosis
Epiphrenic diverticulum.
✓ Pearls
Epiphrenic diverticula typically arise from right posterior–lateral wall.
Hiatal hernia will typically be left sided on radiograph while epiphrenic diverticulum will typically be right sided.
Phrenic ampulla is a normal structure, which can be prominent in some patients.
Suggested Readings
Dean C, Etienne D, Carpentier B, Gielecki J, Tubbs RS, Loukas M. Hiatal hernias. Surg Radiol Anat. 2012; 34(4):291–299 Fasano NC, Levine MS, Rubesin SE, Redfern RO, Laufer I. Epiphrenic diverticulum: clinical and radiographic findings in 27 patients. Dysphagia. 2003; 18(1):9–15 Federle MP, Jeffrey RB, Woodward PJ, Borhani A. Diagnostic Imaging: Abdomen. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009Case 78

Key Finding
Gastric solid mass.
Top 3 Differential Diagnoses
Gastric adenocarcinoma: Adenocarcinoma arises from the gastric epithelium and is the most common gastric malignancy accounting for greater than 95% of malignant stomach tumors. Most occur sporadically. There is an important association with H. pylori infection and about 10 to 15% have a genetic predisposition. Median age is 70 years for males and 74 years for females. Gastric adenocarcinoma can occur anywhere in the stomach but about half the time it presents in the pyloric region and one fourth of the time in the body and fundus. Distal stomach masses may present with gastric outlet obstruction. It can present as gastric focal wall thickening on CT. Other patterns include polypoid mass, ulcerated mass, or infiltrating lesion with loss of normal rugal fold pattern.
Lymphoma: Primary gastric lymphoma represents 1 to 5% of malignant tumors of the stomach. Lymphoma is the second most common gastric malignancy. Ninety percent of primary gastric lymphoma are mucosa associated lymphoid tissue (MALT) or diffuse large B-cell lymphoma (DLBCL). MALT is often associated with H. pylori infection. It is predominately non-Hodgkin’s lymphoma (NHL) type. It is frequently found in the antrum. On CT, lymphoma can present as focal or diffuse wall thickening usually greater than 1 cm, ulcerated polypoid lesions or submucosal nodular form.
Gastric gastrointestinal stromal tumor (GIST): Most common mesenchymal origin neoplasm. The majority of these lesions occur in the stomach. It expresses tyrosine kinase growth factor receptor that distinguishes it from leiomyomas, leiomyosarcoma, schwannoma, and neurofibroma. On CT, GIST presents as a large exophytic, hypervascular mass. Calcifications are present in 5 to 10% of cases. Lymphadenopathy is not seen. GIST has an association with neurofibromatosis type I.
Additional Diagnostic Considerations
Benign gastric polyp: Usually asymptomatic and found incidentally on barium examinations. In rare cases, it may present with epigastric pain, gastric outlet obstruction, and hematemesis. Incidence increases with age. Fundic gland polyps represent 74% of all gastric polyps in Western countries where prevalence of H. pylori is less prevalent. In countries with high prevalence of H. pylori, polyps are usually hyperplastic and adenomas. Fundic gland polyps have a low malignant potential. Adenomas are typically seen in atrophic gastric mucosa and may be associated with familial polyposis syndromes.
Gastric carcinoids: Sporadic gastric carcinoid is a subtype of gastric carcinoid that usually presents as a large solitary lesion (the two other sub types present as multiple small lesions). They are usually metastatic upon diagnosis. In total, all types of gastric carcinoids are rare tumors that comprise 1% of all gastric neoplasms.
Diagnosis
Gastric adenocarcinoma.
✓ Pearls
Gastric adenocarcinoma is the most common stomach malignancy.
Sister Mary Joseph node is an umbilical nodule secondary to metastasis seen in up to 3% of intra-abdominal and pelvic malignancies.
Gastrointestinal tract is most common extranodal site involved by lymphoma.
Suggested Readings
Federle MP, Jeffrey RB, Woodward PJ, Borhani A. Diagnostic imaging: abdomen. 2nd ed. Lippincott Williams & Wilkins; 2009 Lockhead P, El-Omar E. Gastric tumors: an overview. Atlas Genet Cytogenet in Oncol Haematol. 2009; 13(10):761:767 Shen Y, Kang HK, Jeong YY, et al. Evaluation of early gastric cancer at multidetector CT with multiplanar reformation and virtual endoscopy. Radiographics. 2011; 31(1):189–199Case 79

Key Finding
Diffuse thickened small bowel folds.
Top 3 Differential Diagnoses
Inflammatory: Inflammatory processes typically cause irregular fold thickening. The folds become distorted and form angles with adjacent folds. While any inflammatory process can cause this appearance, the key to differentiating them relies on noting the site of disease, provided clinical history and other supportive radiographic findings. For example, Crohn’s disease will show involvement of the terminal ileum along with the “string sign,” separation of bowel loops, skip lesions, and possible fistula formation. Gastric involvement in addition to small bowel can be seen in eosinophilic gastroenteritis. The presence of a malabsorption syndrome such as fever, arthritis, and lymphadenopathy can be seen in Whipple’s disease. Biopsy of the small bowel will show periodic acid–Schiff (PAS)-positive granules in the lamina propria.
Hemorrhage: Hemorrhage causes uniform, regular thickening of the small bowel folds. This can create the classic “picket fence” or “stack of coins” configuration due to the parallel alignment of the small bowel folds. Bowel loops will often show separation as well. This can be caused by multiple reasons including, but not limited to, anticoagulant therapy, connective tissue diseases, coagulation abnormalities, bleeding varices, and hemorrhagic neoplasm.
Edema: Another common cause of regular small bowel thickening. This is most commonly related to hypoproteinemia due to hepatic cirrhosis. Similarly, nephrotic syndrome and protein-losing enteropathies also result in edema. While protein losing diseases typically cause generalized bowel thickening, lymphatic blockage from tumor infiltration and angioneurotic edema will cause a similar fold pattern but typically are more localized.
Additional Diagnostic Considerations
Lymphoma/leukemia: Approximately 25% of patients with lymphoma will have small bowel involvement at autopsy. Lymphomatous/leukemic involvement of the small bowel is typically irregular in nature with diffuse distribution. The bowel loops will show separation due to mesenteric involvement of the disease.
Infection: Irregular thickening of small bowel folds that has a multitude of causes. This includes Giaradiasis (correlate with history of recent travel to an endemic area), Yersinia enterocolitis, Strongyloidiasis, and typhoid fever are other possible etiologies.
Diagnosis
Small bowel hemorrhage related to coagulopathy.
✓ Pearls
Regular diffuse small bowel fold thickening is most likely related to hemorrhage or edema.
Inflammatory conditions are the most common cause of irregular fold thickening.
Narrowing the differential relies on looking on involvement pattern, clinical signs/symptoms, and associated radiologic findings.
Suggested Readings
Eisenberg RL. Thickening of small bowel folds. AJR Am J Roentgenol. 2009; 193(1):W1:W6 Federle MP, Jeffrey RB, Woodward PJ, Borhani A. Diagnostic Imaging: Abdomen. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009 Rubesin SF, Rubin RA, Herlinger H. Small bowel malabsorption: clinical and radiological perspectives. Radiology. 1992; 184:2973Case 80

Key Finding
Right lower quadrant cystic mass with peripheral calcification.
Top 3 Differential Diagnoses
Appendicitis/appendiceal abscess: Appendicitis most commonly presents with periumbilical pain eventually localizing to the right lower quadrant. Classic findings in appendicitis include a dilated appendix measuring greater than or equal to 7 mm with surrounding inflammatory fat stranding, with or without associated free fluid and appendicolith. Complications include rupture with abscess formation and pneumoperitoneum.
Mucocele of the appendix: Most commonly asymptomatic, mucocele of the appendix results from chronic cystic dilation by abnormal mucin accumulation. Three histologic subtypes exist including mucosal hyperplasia, mucinous cystadenoma (most common) and mucinous cystadenocarcinoma. On CT, an encapsulated round or oval, thin walled cystic mass is seen in the right lower quadrant. These most commonly measure 3 to 6 cm and approximately 50% have curvilinear mural calcification. Pseudomyxoma peritonei can be seen with rupture.
Cecal adenocarcinoma: Finding of cecal adenocarcinoma is similar to those of colon neoplasms in other portions of the bowel, often presenting due to hematochezia or bowel obstruction. These masses can be large at presentation. On imaging, there may be signs of transmural invasion, adenopathy, or distant metastasis. Associated inflammatory changes are rare.
Additional Diagnostic Considerations
Adnexal mass: Right lower quadrant pain in women often stems from ovarian or adnexal origin, with possible etiologies including simple or complex ovarian cysts, tubo-ovarian abscess, endometriomas, and both benign and malignant ovarian neoplasms. When large, it may be difficult to localize to the adnexa and can simulate a cecal/appendiceal cystic mass. On cross-sectional imaging following the gonadal artery and broad ligament to the ovary may be helpful in localizing the lesions origin.
Diagnosis
Mucocele of the appendix, mucinous cystadenoma.
✓ Pearls
Enlarged appendix with inflammatory changes less than 2 cm is considered to be appendicitis.
Mucoceles of the appendix present as large cystic masses greater than 3 cm with calcifications.
Pseudomyxoma peritonei is associated with rupture of mucin secreting tumors.
Suggested Readings
Beydoun T, Kreuer S. Cystic right lower quadrant mass. J Am Osteopath Coll Radiol. 2012; 1(4):32–34 Jeong YY, Outwater EK, Kang HK. Imaging evaluation of ovarian masses. Radiographics. 2000; 20(5):1445–1470 Madwed D, Mindelzun R, Jeffrey RB, Jr. Mucocele of the appendix: imaging findings. AJR Am J Roentgenol. 1992; 159(1):69–72 Pickhardt PJ, Levy AD, Rohrmann CA, Jr, Kende AI. Primary neoplasms of the appendix: radiologic spectrum of disease with pathologic correlation. Radiographics. 2003; 23(3):645–662Case 81

Key Finding
Marked rectal distention with fecal impaction and wall thickening.
Top 3 Differential Diagnoses
Stercoral colitis: This is an inflammatory colitis of the rectal wall secondary to fecal impaction (fecaloma) with increased intraluminal pressure. The fecaloma results in rectal and eventual perirectal hazy fat. The rectal wall is thickened diffusely or focally (if stercoral ulcer is present). Complications include perforation /peritonitis with a high mortality rate. Typically, a disease of elderly, chronically disabled, and/or institutionalized patient. In young patient, etiology is primarily narcotic abuse.
Ogilvie syndrome/ileus: Dilated rectum and colon without an obstructive lesion (tumor, infection, or inflammation). Colonic ileus can dilate the rectum but is most prominent in the cecum. Etiologies include trauma, metabolic imbalance, postoperative, infectious, and cardiac disease. Pseudo-obstruction (Ogilvie syndrome) is a potentially fatal condition of acute colonic distention without an underlying mechanical lesion. CT will show luminal distention without an abrupt transition point.
Inflammatory bowel disease: Crohn’s disease and ulcerative colitis both result in bowel wall thickening. Ulcerative colitis is more common in the left colon and Crohn’s disease is more common in the right colon. The wall thickening is more prominent in Crohn’s disease typically greater than 10 mm. Ulcerative colitis complications include colonic stricture or a fixed and dilated colon (lead pipe). Ulcerative colitis classic findings are concentric wall thickening involving the left colon and rectum.
Additional Diagnostic Considerations
Adenocarcinoma: Adenocarcinoma is the most common colorectal malignancy. Typical CT findings are irregular, asymmetric rectal wall thickening, and luminal narrowing. Complications include obstruction proximal to a transition point created by the mass-like wall thickening. It commonly presents with surrounding fat stranding and adenopathy.
Proctitis: An inflammation of the lining of the rectum can be acute or chronic. On cross-sectional imaging, the rectal wall thickening is classically concentric without luminal distention. Etiologies include radiation therapy, sexually transmitted infections, inflammatory diseases, ischemia, and trauma.
Diagnosis
Stercoral colitis.
✓ Pearls
In uncomplicated fecal impaction, rectal wall is thin differentiating this from stercoral colitis.
The rectal wall is thickened in proctitis but without luminal distention, unlike stercoral colitis.
Postoperative patients with distention typically are due to an ileus.
Suggested Readings
Boyd SK, Cameron-Morrison JD, Hobson JJ, Saenz R. CT imaging of large bowel wall thickening. J Am Osteopath Coll Radiol. 2016; 5(2):14–22 Choi JS, Lim JS, Kim H, et al. Colonic pseudoobstruction: CT findings. AJR Am J Roentgenol. 2008; 190(6):1521–1526 Heffernan C, Pachter HL, Megibow AJ, Macari M. Stercoral colitis leading to fatal peritonitis: CT findings. AJR Am J Roentgenol. 2005; 184(4):1189–1193Case 82

Key Finding
Eccentric wall thickening of the distal esophagus.
Top 3 Differential Diagnoses
Esophageal carcinoma: The most common type of esophageal carcinoma is squamous cell carcinoma (SCC). SCC is typically seen in the proximal two-thirds while adenocarcinoma is more commonly seen in the distal One-thirds. Adenocarcinoma is the second most common type of cancer. Both can present as either circumferential or asymmetric wall thickening. Mediastinal lymphadenopathy suggests localized metastasis. Risk factors for esophageal SCC include tobacco use, alcohol consumption, achalasia, and long standing esophagitis. Adenocarcinoma is more closely related with gastroesophageal reflux and Barrett’s metaplasia.
Esophagitis: Inflammation of the esophagus most commonly caused by gastroesophageal reflux but can also be secondary to infection, chemotherapy, caustic ingestion, or radiation. CT may demonstrate wall thickening, submucosal edema (target sign), and thickened folds. Esophagus may demonstrate a “shaggy” appearance on barium studies.
Esophageal varices: Dilated and tortuous collateral veins which may be “uphill” due to increased portal venous pressure or “downhill” due to superior vena cava (SVC) obstruction. Varices may present on CT as wall thickening with a lobular contour. Tortuous radiolucent filling defects can be seen on barium esophagram. Variceal hemorrhage is the most serious complication. Treatment may include blood pressure control or vascular ligation. Transjugular intrahepatic portosystemic shunt (TIPS) can be performed to relieve portal hypertension. Varicoid carcinoma should be considered if the esophagus demonstrates a varicoid appearance and does not distend with contrast administration.
Additional Diagnostic Considerations
Lymphoma and metastasis: Metastasis of the esophagus is most commonly by direct spread, although lymphatic or hematogenous spread is also possible. Gastric and lung cancers are most common primaries with esophageal metastasis. Lymphoma involving the esophagus is most commonly due to non-Hodgkin. The esophagus is the least commonly affected portion of the gastrointestinal tract by lymphoma. Primary esophageal lymphoma may be seen in AIDS patients.
Diagnosis
Esophageal adenocarcinoma.
✓ Pearls
SCC is more strongly associated with smoking and alcohol use. SCC is typically seen in proximal two-third of esophagus.
Adenocarcinoma is more often a result of chronic gastroesophageal reflux disease (GERD) with progression to Barrett’s esophagus and adenocarcinoma. It is more often seen in distal one-third of esophagus.
Esophageal varices may be “downhill” or “uphill” and present as serpiginous filling defects. Varicoid carcinoma should be considered if the esophagus does not distend.
The esophagus is the portion of the gastrointestinal tract least commonly affected by lymphoma. Direct invasion from lung or gastric carcinoma represent the most common esophageal metastases.
Suggested Readings
Bhalla M, Silver RM, Shepard JA, McLoud TC. Chest CT in patients with scleroderma: prevalence of asymptomatic esophageal dilatation and mediastinal lymphadenopathy. AJR Am J Roentgenol. 1993; 161(2):269–272 Federle MP, Jeffrey RB, Woodward PJ, Borhani A. Diagnostic Imaging: Abdomen. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009 Hong SJ, Kim TJ, Nam KB, et al. New TNM staging system for esophageal cancer: what chest radiologists need to know. Radiographics. 2014; 34(6):1722–1740 Reinig JW, Stanley JH, Schabel SI. CT evaluation of thickened esophageal walls. AJR Am J Roentgenol. 1983; 140(5):931–934Case 83

Key Finding
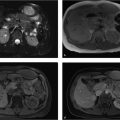
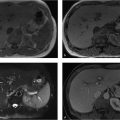
Lesion posterior to the stomach.
Top 3 Differential Diagnoses
Gastric diverticulum: Gastric diverticulum is not uncommon. The most common location is in the cardiac region. The key to the diagnosis is visualizing the connection of the diverticulum to the stomach. This may be confirmed on CT with oral contrast or barium fluoroscopy. Typically these are true diverticula and extend through all three layers of the stomach wall.
Adrenal mass: The most common mass of the adrenal gland is an adenoma. Adenomas account for greater than 90% of adrenal masses. The second most common cause of adrenal lesions is metastasis. Adrenal pheochromocytomas are hypervascular lesions that are typically greater than 3 cm in size. Adrenal primary carcinomas are usually large lesions greater than 6 cm in size. CT adrenal washout studies have the highest sensitivity for differentiating adenomas from metastasis.
Accessory spleen: It represents benign splenic tissue that is congenital origin. The most common location of it is around the hilum of the spleen. The key to diagnosis is noting the same attenuation on CT or signal intensity on MRI as the native spleen. Approximately 10 to 30% of patients have accessory spleens. An accessory spleen can hypertrophy after splenectomy.
Diagnosis
Gastric diverticulum.
✓ Pearls
Gastric diverticulum can be confirmed on a barium study with contrast filling.
An air-fluid level in a posterior gastric mass is a diverticulum.
Adrenal adenomas that are lipid rich are easily diagnosed on MRI chemical shift imaging.
Suggested Readings
Federle MP, Jeffrey RB, Woodward PJ, Borhani A. Diagnostic Imaging: Abdomen. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009 Schwartz AN, Goiney RC, Graney DO. Gastric diverticulum simulating an adrenal mass: CT appearance and embryogenesis. AJR Am J Roentgenol. 1986; 146(3):553–554Case 84

Key Finding
Dilated small bowel loops.
Top 3 Differential Diagnoses
Mechanical obstruction: Dilated small bowel loops are greater than 2.5 cm in diameter when measuring from outer wall to outer wall. Stacked air-fluid levels are seen on the upright abdominal film. CT is utilized to further characterize the degree of obstruction (low-grade partial, high-grade partial or complete) and to identify a transition point to aid in surgical planning. Small bowel follow-through is typically used to aid in partial versus complete obstruction characterization although delayed CT after the administration of oral contrast has accomplished similar results in the literature. The most common causes are overwhelmingly postsurgical adhesions (developed world) and hernias (developing world).
Ileus: A term used to describe aperistaltic bowel not caused by mechanical obstruction. Radiographically it can be difficult to distinguish from mechanical obstruction as many features overlap. Clinical information can aid in differentiation as patients will typically present with non-colicky abdominal pain, which is prolonged and often occurs after surgery. CT will also demonstrate lack of a transition point and lack of distal decompressed loops of small and large bowel. Medications have been implicated as well, most commonly opioids.
Scleroderma: Results in systemic sclerosis due to the deposition of collagen. In addition to small bowel dilatation, can cause reversal of jejunal/ileal fold pattern that is caused by villous atrophy and crypt hypertrophy leading to chronic fluid overload. Classically it is seen with sacculations along with antimesenteric border. Look for associated imaging findings such as esophageal dilatation and pulmonary fibrosis.
Additional Diagnostic Considerations
Sprue: Sprue results in lack of mucosal folds in the jejunum. This leads to a featureless appearance of the jejunum, which then appears as a “cast” of itself which is termed the “Moulage sign.”
Diagnosis
Small bowel obstruction.
✓ Pearls
Small bowel is dilated when it is larger than 2.5 cm.
Look for a transition point and distal decompressed small bowel loops to differential mechanical obstruction from an ileus.
Inflammatory conditions resulting in small bowel dilatation will have other radiographic signs to aid in the diagnosis.
Suggested Readings
Federle MP, Jeffrey RB, Woodward PJ, Borhani A. Diagnostic Imaging: Abdomen. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009 Lappas JC, Reyes BL, Maglinte DD. Abdominal radiography findings in small-bowel obstruction: relevance to triage for additional diagnostic imaging. AJR Am J Roentgenol. 2001; 176(1):167–174 Silva AC, Pimenta M, Guimarães LS. Small bowel obstruction: what to look for. Radiographics. 2009; 29(2):423–439Case 85

Key Finding
Asymmetric cecal wall thickening.
Top 3 Differential Diagnoses
Adenocarcinoma: Adenocarcinoma is the most common carcinoma of the colon. The cecum accounts for 25% of all adenocarcinomas within the colon. In the cecum, they can grow to be large without causing obstruction and can serve as lead points for intussusception. CT features include asymmetric wall thickening within a shorter segment of bowel, abrupt change from abnormal to normal bowel wall, and minimal adjacent fatty infiltration. When large, these masses can be bulky and polypoid. In 10% of cases, these cecal masses can extend and involve the terminal ileum and result in congestion and edema of the terminal ileum. On barium evaluations, luminal narrowing is identified.
Diverticulitis: Diverticular disease is most common in the distal colon and less common in the cecum. Identification of cecal diverticuli, asymmetric or circumferential bowel wall thickening, and pericecal inflammatory change are key CT findings. Visualization of a normal appendix and pericolonic inflammation at the site of the cecal diverticula excludes appendicitis. Complications include perforation with pneumoperitoneum and abscess formation.
Infectious colitis: Infections result in focal or diffuse bowel wall thickening with ulcerations. Certain organisms are known to affect the right colon with occasional spread to the terminal ileum and the possibility of affecting the distal colon. These are salmonellosis (typhoid fever), Yersinia enterocolitis, tuberculosis, cytomegalovirus (CMV), histoplasmosis, mucormycosis, and amebiasis. CT may show thickened folds and wall thickening, haustral loss from edema or spasm, ulcerations, and narrowing of the lumen. Each organism may cause a slightly different appearance within the segments involved.
Additional Diagnostic Considerations
Inflammatory disease: Crohn’s disease affects the terminal ileum and the cecum. Skip lesions with wall thickening, wall edema with layered enhancement, mesenteric fat stranding, and lymph nodes are identified within the acute stage of the disease. Complications of fistula formation, sinus tracts, and abscesses are also noted. Ulcerative colitis is a pancolitis involving the entire colon from the rectum to the cecum. Decreased haustrations and ulcerations on barium enema examinations are noted. The risk of colon carcinoma is greater in ulcerative colitis than in Crohn’s disease with 25% of ulcerative colitis cases having multiple carcinomas.
Lymphoma: The cecum is the most common location of primary lymphoma in the colon with possible extension to involve the terminal ileum and the appendix. Single or multiple segments of more symmetric circumferential wall thickening with marked wall thickening (1.5–7 cm) is identified. Aneurysmal dilation of the bowel and ulceration with fistulous communication with other bowel loops are potential complications. Significant lymphadenopathy can also be identified.
Diagnosis
Adenocarcinoma.
✓ Pearls
Carcinomas in the cecum when large may be lead points for intussusception.
Crohn’s disease is more common along the right colon while ulcerative colitis is more common along the left colon and rectum.
Diverticulitis should only be considered when diverticula are present.
Suggested Readings
Boyd SK, Cameron-Morrison JD, Hobson JJ, et al. CT imaging of large bowel wall thickening. J Am Osteopath Coll Radiol. 2016; 5(2):14–22 Federle MP, Jeffrey RB, Woodward PJ, Borhani A. Diagnostic Imaging: Abdomen. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009 Hoeffel C, Crema MD, Belkacem A, et al. Multi-detector row CT: spectrum of diseases involving the ileocecal area. Radiographics. 2006; 26(5):1373–1390Case 86

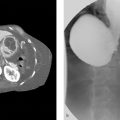
Clinical History
A 74-year-old female with a urinary tract infection with remote history of hysterectomy (▶Fig. 86.1).
Key Finding
Air in the urinary bladder in absence of a catheter.
Top 3 Differential Diagnoses
Diverticulitis: Diverticulitis is the most common cause of colovesical fistula formation and is associated with approximately half of cases. While more common in men, overall there is an increased risk in women following hysterectomy. The fistula tract is rarely seen directly. Indirect findings of a colovesical fistula include intravesicular air with focal bladder wall thickening and/or inflammatory changes of the colon with loss of the fat plane between the colon and the urinary bladder. Occasionally, cystography or a contrast enema may demonstrate the fistulous tract.
Recent instrumentation: Air can be introduced into the urinary bladder with instrumentation, most commonly following introduction or removal of a catheter. The presence of a Foley catheter bulb within the bladder lumen accounts for vesicular air. The lack of urinary bladder wall thickening and absence of perivesicular fat stranding excludes inflammation.
Cystitis: When infection of the bladder occurs in the presence of gas forming bacteria, intravesicular air and urinary bladder wall thickening can be seen simulating a fistula. On CT, look for perivesicular fat stranding without involvement of the surrounding bowel.
Additional Diagnostic Considerations
Inflammatory bowel disease: Fistula formation is a known complication of Crohn’s disease. While it most commonly involves the terminal ileum any portion of bowel can be involved. In addition to secondary signs of colovesical fistula, classic findings of Crohn’s disease may be seen including circumferential bowel wall thickening often with skip lesions, mesenteric hyperemia, fatty infiltration of the bowel wall, and strictures.
Neoplasm/carcinoma: Both genitourinary and gastrointestinal neoplasms have been associated with colovesical fistulas. On CT, indirect signs of fistula can be seen including air within the urinary bladder. There will be associated bladder and/or colonic wall thickening in the absence of surrounding inflammatory change. Lymphadenopathy may also be seen.
Diagnosis
Colovesical fistula secondary to diverticulitis.
✓ Pearls
Correlate for history of recent instrumentation when air is seen within the bladder.
Hysterectomy increases the risk of colovesical fistula formation in women.
A direct fistulous tract is rarely seen, so secondary signs are helpful.
Suggested Readings
Boyd SK, Cameron-Morrison JD, Hobson JJ, Saenz R. CT imaging of large bowel wall thickening. J Am Osteopath Coll Radiol. 2016; 5(2):14–22 Federle MP, Jeffrey RB, Woodward PJ, Borhani A. Diagnostic Imaging: Abdomen. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009 Yu NC, Raman SS, Patel M, Barbaric Z. Fistulas of the genitourinary tract: a radiologic review. Radiographics. 2004; 24(5):1331–1352Case 87

Key Finding
Transverse esophageal folds/lines.
Top 3 Differential Diagnoses
Feline esophagus: Transverse esophageal lines involving the entire circumference of the esophagus. The esophageal markings are transient in nature, thin (1–2 mm), and almost always seen in association with gastroesophageal reflux. Feline esophagus is named after the morphologic similarity to a cat’s esophagus. The transverse folds typically resolve during swallowing.
Esophageal web: A mucosal fold resulting in variable degree of esophageal narrowing. It often appears as a thin (1–2 mm wide) shelf-like filling defect but can also appear as a circumferential radiolucent ring. Webs are usually asymptomatic and may be seen anywhere throughout the esophagus. Webs are most common within the upper cervical esophagus. Esophageal webs have several associated conditions including chronic gastroesophageal reflux, Plummer–Vinson syndrome, chronic gastroesophageal reflux, and eosinophilic esophagitis.
Diffuse esophageal spasm (DES): DES results in irregular esophageal motility that can cause noncardiac chest pain or dysphagia. The key imaging features on fluoroscopy include transverse bands and nonperistaltic contractions with both anterograde and retrograde movement of contrast. Transverse bands will be larger in size when compared to the feline esophagus. These can uncommonly result in a classic “corkscrew” or “rosary bead” esophagus.
Additional Diagnostic Considerations
Eosinophilic esophagitis: Inflammation of the esophagus with characteristic infiltration of eosinophils. Most characteristic imaging finding is concentric esophageal strictures on barium swallow (ring esophagus). It can be seen anywhere along the gastrointestinal tract and may manifest as fold thickening and submucosal edema within the bowel. Most of those affected have allergy/food intolerance history. Biopsy of esophagus is required for definitive diagnosis. Eosinophilic esophagitis responds well to steroid treatment.
Diagnosis
Feline esophagus.
✓ Pearls
Feline esophagus is almost always associated with gastroesophageal reflux. It is transient and will resolve during swallowing.
Larger transverse folds with bidirectional movement on contrast suggest DES.
Esophageal webs are associated with esophagitis, Plummer–Vinson syndrome, and chronic reflux.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


