Part 5 Abdominal Wall and Soft Tissues
Case 141
Key Finding
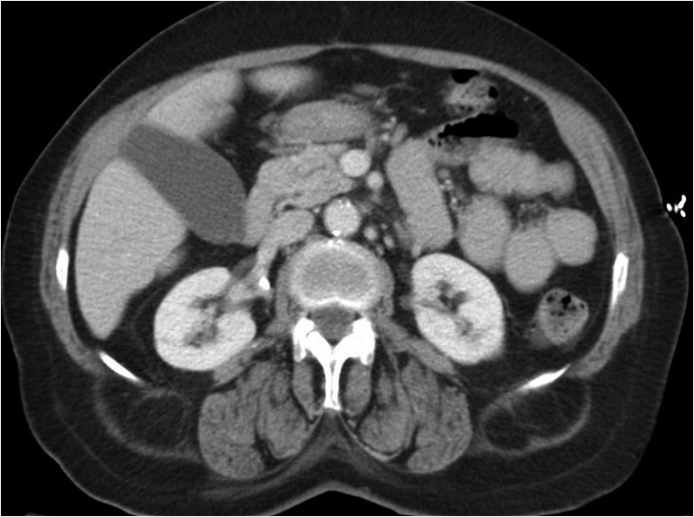
Retroperitoneal fat herniating though the posterior abdominal wall.
Top 3 Differential Diagnoses
Lumbar hernia: Lumbar hernia is a hernia through the lumbar triangle. Lumbar hernias can contain essentially any retroperitoneal organ. These are divided into superior and inferior lumbar triangle hernias. Superior hernias are also known as Grynfeltt–Lesshaft and inferior hernias are also called Petit’s hernias. The superior hernias are more common. These occur between the quadratus lumborum, 12th rib, and the internal oblique muscle. The boundaries of the inferior hernias consist of the iliac crest, external abdominal oblique muscles, and the margins of the latissimus dorsi muscle. Acute abdominal trauma more commonly results in Petit’s hernias. Both superior and inferior hernias may be related to incisions from a recent procedure. Secondary to the large size of lumbar hernias, it is uncommon for associated incarceration and strangulation of herniated bowel.
Congenital diaphragmatic hernia: Congenital diaphragmatic hernias include Bochdalek hernias, which are the most common type of congenital diaphragmatic hernia, and involve the posterior–lateral aspect of the diaphragm and typically present in infancy. Another type of congenital diaphragmatic hernia is a Morgagni hernia, which involves the anterior aspect of the diaphragm and typically presents later in life. Traumatic diaphragmatic hernia typically occurs after trauma and causes abdominal or retroperitoneal structures to herniate into the chest cavity secondary to the negative intrathoracic pressure. There is a high association of intra-abdominal organ injury with traumatic diaphragmatic rupture.
Abdominal wall lipoma: Lipomas are benign fatty tumors that can occur anywhere in the body. These tumors follow fat on all cross-sectional studies. These lesions are typically incidentally found. On MRI, fat saturation sequences are helpful to solidify the diagnosis. Imaging findings of lipomas that suggest liposarcoma include nodules of soft tissue and foci of enhancement.
Diagnosis
Superior lumbar hernia, Grynfeltt–Lesshaft.
✓ Pearls
Grynfeltt–Lesshaft hernias are uncommon to cause bowel strangulation.
Petit’s hernias occur just above the iliac crest.
Nodular enhancement of a lipoma raises the concern for liposarcoma.
Suggested Readings
Aguirre DA, Santosa AC, Casola G, Sirlin CB. Abdominal wall hernias: imaging features, complications, and diagnostic pitfalls at multi-detector row CT. Radiographics. 2005; 25(6):1501–1520 Federle MP, Jeffrey RB, Woodward PJ, Borhani A. Diagnostic Imaging: Abdomen. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009 Killeen KL, Girard S, DeMeo JH, Shanmuganathan K, Mirvis SE. Using CT to diagnose traumatic lumbar hernia. AJR Am J Roentgenol. 2000; 174(5):1413–1415Case 142
Key Finding
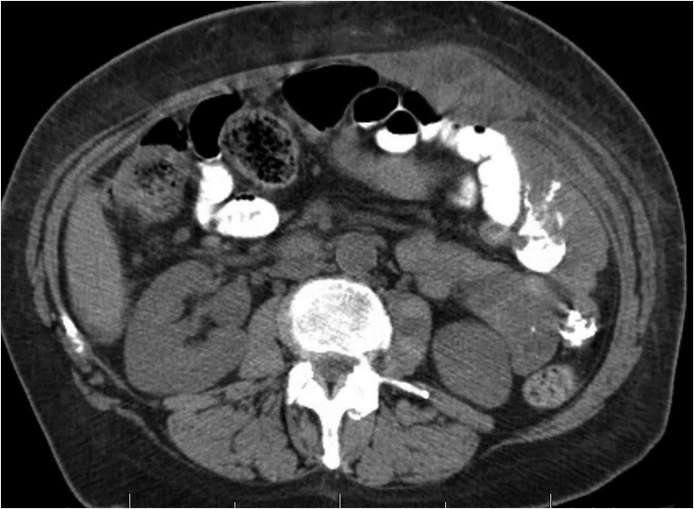
Enlargement of the abdominis rectus.
Top 3 Differential Diagnoses
Hematoma: In a patient with history of trauma or anticoagulation use, hematoma is the most common etiology. On noncontrast CT, a hematoma can appear to be isoattenuating to the muscle but can be of higher attenuation with acute bleeding. While there is lack of enhancement on contrast-enhanced CT, focal hyperattenuation within the hematoma can represent active extravasation. Follow-up imaging will show regression. MR appearance is variable due to different appearances of blood products over time.
Abscess: On contrast-enhanced CT, this can be seen as a low-density fluid collection with a peripherally enhancing rim. With MRI, appearance is variable and depends on its internal contents. Typically, it has high T2 signal that becomes more heterogeneous with increasing amounts of necrosis, debris, or gas.
Neoplasm: Usually tumors demonstrate enhancement when compared to precontrasted images. Tumors that may involve the rectus abdominis include, but not limited to, lipoma, desmoid, fibrous tumor, metastasis, or lymphoma.
Additional Diagnostic Considerations
Endometriosis: Endometriomas are hemorrhagic cysts, resulting from functioning endometrium outside of the uterus. The abdominal wall is the most common site of extrapelvic involvement. Classic presentation is an abdominal wall mass near a C-section scar in a patient with cyclical pain. On MRI, endometriomas appear hyperintense on T1-weighted image, but demonstrate hypointense signal on T2-weighted image known as “T2 shading.”
Ventral hernia: These hernias occur through the linea alba of the abdominal wall and are in the midline. On physical examination, hernias can be confused for soft-tissue masses. On imaging, the diagnosis is obvious when the “mass” is noted to be contiguous with the bowel. CT is useful to evaluate obstruction, incarceration, strangulation, and necrosis.
Diagnosis
Rectus abdominis hematoma
✓ Pearls
Hematoma is the most common cause of a rectus abdominis mass, it is strongly associated with trauma or use of anticoagulation.
Consider endometrioma in a female with an abdominal wall mass that enlarges with menses.
An abdominal wall abscess may have a fistulous connection to the bowel (oral contrast may be beneficial in the diagnosis).
Suggested Readings
Gidwaney R, Badler RL, Yam BL, et al. Endometriosis of abdominal and pelvic wall scars: multimodality imaging findings, pathologic correlation, and radiologic mimics. Radiographics. 2012; 32(7):2031–2043 Stein L, Elsayes KM, Wagner-Bartak N. Subcutaneous abdominal wall masses: radiological reasoning. AJR Am J Roentgenol. 2012; 198(2):W146–51Case 143
Clinical History
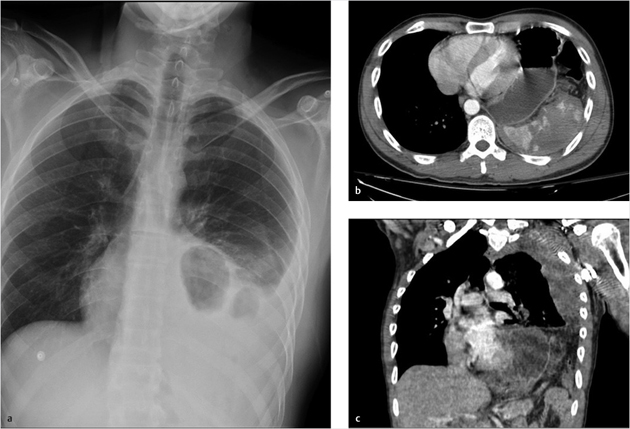
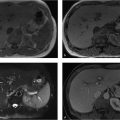
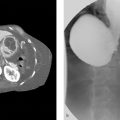
A 31-year-old male with left upper quadrant pain after a motor vehicle accident (▶Fig. 143.1).
Key Finding
Diaphragmatic attenuation.
Top 3 Differential Diagnoses
Congenital diaphragmatic hernia: Congenital diaphragmatic hernias include Bochdalek hernias, which are the most common type of congenital diaphragmatic hernia, and involve the posterior–lateral aspect of the diaphragm and typically present in infancy. Another type of congenital diaphragmatic hernia is a Morgagni hernia, which involves the anterior aspect of the diaphragm and typically presents later in life. Traumatic diaphragmatic hernia typically occurs after trauma and causes abdominal or retroperitoneal structures to herniate into the chest cavity secondary to the negative intrathoracic pressure. There is a high association of intra-abdominal organ injury with traumatic diaphragmatic rupture.
Traumatic diaphragmatic hernia: Traumatic diaphragmatic hernia or diaphragmatic rupture typically occurs after significant abdominal trauma. The abdominal or retroperitoneal structures herniate into the chest cavity secondary to the negative intrathoracic pressure. There is a high association of intra-abdominal organ injury with traumatic diaphragmatic rupture. The most common location is on the left.
Hiatal hernia: It is a type of acquired hernia that occurs when abdominal structures herniate through the esophageal hiatus, typically the stomach. This can be differentiated from other types of diaphragmatic hernias by its central location and involvement of the esophageal hiatus. There are two types of hiatal hernias: sliding and paraesophageal. Sliding is the most common type of hiatal hernia and occurs when the gastroesophageal junction herniates above the esophageal hiatus, whereas the paraesophageal hiatal hernia occurs when the gastroesophageal junction remains within the normal location and a portion of the stomach herniates through the hiatus.
Additional Diagnostic Considerations
Congenital pulmonary airway malformation (CPAM): It is a congenital lung lesion that can mimic diaphragmatic hernia on a chest radiograph secondary to its multicystic properties. CPAM is usually diagnosed within the antenatal period and may present with respiratory distress and pulmonary hypoplasia, although it may present into adulthood. Cross-sectional imaging is critical and will demonstrate an intact diaphragm.
Pericardial cyst: Pericardial cysts occur within the cardiophrenic recess and are more common on the right side. Pericardial cysts arise from the pericardium and may mimic a diaphragmatic hernia on a chest radiograph, but are easily differentiated on cross-sectional imaging secondary to the well-defined and uniformly low-attenuated fluid pericardial cyst arising from the pericardium.
Diagnosis
Traumatic diaphragmatic hernia/rupture
✓ Pearls
There is a high association of intra-abdominal organ injury with traumatic diaphragmatic rupture.
Diaphragmatic injuries/ruptures are most common on the left side.
Pericardial cysts may mimic a diaphragmatic hernia and are more common on the right side.
Suggested Readings
Biyyam DR, Chapman T, Ferguson MR, Deutsch G, Dighe MK. Congenital lung abnormalities: embryologic features, prenatal diagnosis, and postnatal radiologic-pathologic correlation. Radiographics. 2010; 30(6):1721–1738 Iochum S, Lu, dig T, Walter F, Sebbag H, Grosdidier G, Blum AG. Imaging of diaphragmatic injury: a diagnostic challenge? Radiographics. 2002; 22(Spec No):S103–S116, discussion S116–S118 Pineda V, Andreu J, Cáceres J, Merino X, Varona D, Domínguez-Oronoz R. Lesions of the cardiophrenic space: findings at cross-sectional imaging. Radiographics. 2007; 27(1):19–32Case 144
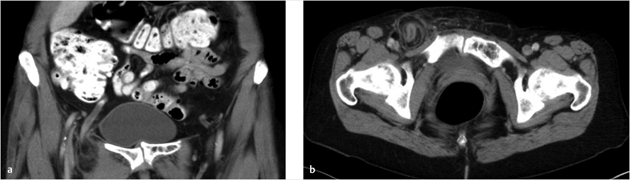
Key Finding
Appendix with an inguinal hernia.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


