Chapter 178
Parotid Duct Calculus
Epidemiology
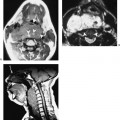
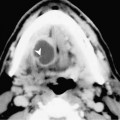
The main parotid (Stensen’s) duct courses anteriorly over the masseter muscle, turns medially into the buccal space, and penetrates the buccinator muscle. The duct opens opposite the second upper molar tooth. Most stones in the parotid gland are solitary but multiple stones or calcifications are often encountered in patients with chronic infection. Chronic infection may be secondary to recurrent bacterial infection or granulomatous disease such as tuberculosis.
Clinical Findings
Patients usually present with a history of repeated episodes of acute sialadenitis. There are intervening asymptomatic periods associated with a decrease in the size of the parotid gland. Some patients may, however, present with a slowly enlarging gland with episodes of acute infection. Physical examination reveals an enlarged parotid gland, which may be tender. A dilated parotid duct, which is usually due to a stone in the orifice of Stensen’s duct or accessory parotid tissue, may rarely appear as a mass in the buccal space.
Pathology
Chronic recurrent sialadenitis is usually secondary to incomplete ductal obstruction as a result of sialolithiasis or strictures from previous suppuration. Repeated episodes of infection often lead to destruction of the glandular acini and multiple small abscesses.
Treatment