The prevalence of tuberculosis (TB) has increased in developing and developed countries as a consequence of the AIDS epidemic, immigration, social deprivation, and inadequate TB control and screening programs. Spinal TB may be osseous or nonosseous. Classic findings of multiple contiguous vertebral body involvement, gibbus formation, and subligamentous spread with paravertebral abscesses are optimally evaluated with MR imaging. Nonspondylitic spinal TB is less well described in the literature, may develop in the absence of TB meningitis, and is often associated with meningovascular cord ischemia. Radiologists should be familiar with the spectrum of imaging findings, allowing early diagnosis and treatment of this serious condition.
Key points
- •
The spine is involved in up to 50% of skeletal TB cases, often presenting with advanced disease as a result of the indolent nature of the infection and low index of suspicion of the diagnosis of TB in non–TB endemic areas.
- •
Nonosseous TB may involve the cord, cauda equine, and/or the meninges.
- •
MR imaging is the imaging modality of choice in the evaluation of spinal TB and should include the whole spine, to assess for multilevel noncontiguous spinal disease.
- •
Including the chest and abdomen in the MR imaging aids in the diagnosis by identifying extraspinal sites of TB.
Historical perspective
In 1782, the English surgeon Sir Percivall Pott described the clinical presentation, examination, and pathologic findings of tuberculous spondylitis (TBS). A century later, the German physician and microbiologist Robert Koch would isolate the causative organism and receive the Nobel Prize in 1905.
Historical perspective
In 1782, the English surgeon Sir Percivall Pott described the clinical presentation, examination, and pathologic findings of tuberculous spondylitis (TBS). A century later, the German physician and microbiologist Robert Koch would isolate the causative organism and receive the Nobel Prize in 1905.
Pathogenesis
Vertebral infection results from dissemination of the tuberculous bacilli from a distant active source or as a result of latent reactivation. Tuberculous involvement of the vertebral body may be paradiscal, anterior subperiosteal, central, or appendiceal. Emphasis has been placed on the normal vascular anatomy of the spine to explain differences in the patterns of infection in children and adults and pyogenic spondylitis versus TBS.
The arterial supply of the vertebral column arises from segmental branches of the vertebral, subclavian, intercostal, and lumbar arteries. Intraosseous arteries arise from two sets of vessels, one anteriorly on the vertebral surface and the other within the spinal canal. Zoned vascular territories have been proposed: the central core of the vertebral body extending from disk to disk supplied by the equatorial arteries, an annular region near the end plate by the metaphyseal arteries, and a surrounding collar from disk to disk supplied by the penetrating arteries.
During the second trimester the intervertebral regions of the spine are avascular. Later in fetal life there is centripetal vascular growth from the periphery and centrifugal vessel growth from the ossification centers. This active vascularization results in an extensive intraosseous anastomotic network in the infantile vertebral body and annulus fibrosis. The nucleus pulposis in contradistinction is never vascular. Vascularity diminishes and disappears entirely by the third decade of life resulting in intraosseous end-arteries. Although these differences may be important determinants in the pathogenesis of pyogenic spine infection, their importance in TBS is less clear. The valveless craniospinal venous plexus of Batson has received recent attention as a potential route of disease and tumor spread and has been implicated in the development of noncontiguous TBS. The central vertebral body pattern of tuberculous infection could be attributable either to the centrally located basivertebral veins or the equatorial arteries.
Pathology
Up to one-half of all musculoskeletal tuberculosis (TB) affects the spine, most commonly in the thoracic and upper lumbar levels. Once the tuberculous bacilli reach the vertebral body or end plate, either hematogenously, via the lymphatics, or directly, in the absence of adequate cell-mediated immunity, active bone destruction (spondylitis) may result. Alternatively there may be partial containment with latent granuloma formation and subsequent reactivation.
The hallmark of TB is the presence of granulomatous inflammation with caseous necrosis. Phagocytosis of the organisms by macrophages results initially in granuloma formation. Central caseation and granuloma breakdown are responsible for release of bacilli into the extracellular space. Once the disease process is no longer confined, extracellular multiplication of bacilli and caseous liquefaction result in destructive spread into the neighboring tissues.
Bone destruction and adjacent tissue necrosis form what has become known as a “pseudo” or “cold” abscess (as distinct from the true polymorph dominant abscess cavity of pyogenic infection) in a high proportion of adult and pediatric patients. Spread to the extraosseous tissues is typically subjacent to the anterior and posterior longitudinal ligaments, paravertebral soft tissues, intervertebral disk, or spinal canal. Paravertebral masses may become very large and displace abdominal organs causing compressive changes in adjacent vertebral bodies. Epidural soft tissue masses are present in 60% to 93% with associated displacement of the thecal sac and compression of the cord or cauda equina. Fistulization to distant sites is common.
Posterior vertebral element involvement, especially isolated disease, is less common. Pedicle involvement as a late and secondary occurrence has been demonstrated in 68% in adults and, in our experience, 85% of children. The average number of contiguous bodies affected (two to three) and the occurrence of noncontiguous disease (<20%) are similar in children and adults and do not seem to be influenced by immune compromise. Sparing of the intervertebral disk in TB was thought to be a classic feature and one that distinguishes TBS from pyogenic spondylitis. More recently with the availability of MR imaging it is clear that disk destruction is common at presentation in TBS, although it remains true that subligamentous extension between adjacent bodies is the primary mode of spread. Local bony destruction and subligamentous decompression may be so extensive that one or more vertebral bodies and their adjacent disks are subsumed in the abscess giving the false impression of disk sparing.
The kyphotic curvature of the spine (gibbus) described by Pott is explained by anterior vertebral body collapse. The exact reason for this is conjectural. Kyphosis may be associated with a combination of epidural pseudoabscess, bony sequestrate, retropulsed sequestered disk, vertebral subluxation/dislocation, and concertina collapse. Less commonly there may be associated penetration of the dura with meningovascular cord compromise. Neurologic deficit tends to occur late in TBS because of the rather slow increase in pressure on the neural axis. Paraplegia may occur without significant kyphosis when there is mechanical instability or vascular compromise.
Clinical presentation
In a large study of 694 adult patients the commonest presenting complaint was paraplegia and/or spinal deformity (70%). Back pain and fever were less frequent (20%). In children the symptoms are commonly nonspecific including torticollis, refusal to weight bear, limp, pain, and palpable mass. It should be remembered that back pain in a child is a red flag necessitating MR imaging. The diagnosis of TB can be suggested on imaging but treatment requires identification of the tuberculous bacillus, and isolation of drug sensitivities ( Box 1 ).
- •
Mantoux tuberculin skin test (in children and unexposed adults).
- •
Ziehl-Neelsen stain for acid-fast bacilli.
- •
Culture for Mycobacterium tuberculosis in Lowenstein-Jensen culture medium (may take up to 8 weeks).
- •
The Xpert MTB/RIF detects DNA sequences specific for M tuberculosis and rifampicin resistance by polymerase chain reaction in sputum in <2 hours. Research into its value in nonsputum analysis is promising.
- •
Histology: caseous granuloma with acid-fast bacilli is diagnostic. Granuloma without acid-fast bacilli is suggestive in the correct clinical context.
Imaging findings
Radiographs of the Spine
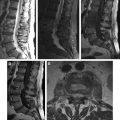
Despite being the mainstay of diagnosis, particularly in resource-limited settings, radiography has disadvantages. More than 50% of the vertebral body needs to be destroyed before changes are evident; this may take up to 6 months from the time of infection. Visualization is limited at the atlanto-occipital, cervicothoracic ( Fig. 1 ), and lumbosacral junctions ( Fig. 2 ) and the posterior elements are often poorly seen. The number of affected vertebral bodies may be underestimated and paraspinal masses or abscesses are often overlooked. Plain film findings range from normal to complete loss of vertebral height (vertebra plana), a rare finding thought to be secondary to central body lysis and found more commonly in children ( Fig. 3 ). Subligamentous extension and paravertebral collections may cause scalloping and erosion ( Fig. 4 ) of the vertebral bodies, and the prevertebral soft tissue associated with high cervical spondylitis may mimic a retropharyngeal collection ( Fig. 5 ). Thoracic paraspinal abscess may be difficult to distinguish from the descending aorta ( Fig. 6 ). Examination of the psoas outlines may reveal asymmetry ( Fig. 7 ) and in chronic cases peripheral calcification that is pathognomonic of TB ( Fig. 8 ). Radiographic progression of bone destruction may continue for up to 14 months after initiation of effective chemotherapy and should not be taken as a sign of treatment failure. Reactive sclerosis and periosteal reaction occur only late or following treatment.
Computed Tomography
Computed tomography (CT) is superior to radiography in demonstrating bone involvement and soft tissue changes and in showing subtle soft tissue calcification. It is more widely available than MR imaging and may be useful in the setting of acute myelopathy. Widening the field of view to include the chest has the advantage of detecting changes of TB that may not be appreciated on the plain film, particularly the tree-in-bud appearance of early alveolar involvement, small pleural effusions, and small-volume lymphadenopathy ( Fig. 9 ). Epidural soft tissue and spinal canal compromise are visible to the astute observer, although cord detail and bone edema cannot be assessed. CT with multiplanar reformats reveals the anatomic extent of bone destruction, particularly involvement of the posterior elements leading to instability, and are invaluable for surgical planning. CT-guided percutaneous biopsy and abscess drainage ( Fig. 10 ) offer an alternative to the open surgical approach, although the radiation dose is of concern particularly in children.
Nuclear Medicine
Technetium-99m diphosphonate bone scans are sensitive but nonspecific in the depiction of spondylodiskitis and are poor at delineating the concomitant soft tissue extent. Fluorodeoxyglucose PET does not provide improved specificity but demonstrates reasonable correlation with C-reactive protein as a measure of activity. It does not perform as well as MR imaging in differentiating between TB and pyogenic spondylitis.
MR Imaging
MR imaging is the imaging modality of choice in the assessment of TBS. It avoids the use of ionizing radiation and its inherent soft tissue contrast demonstrates masses, disks, and spinal cord to advantage. The entire spine should be imaged to exclude multilevel noncontiguous involvement ( Fig. 11 ). A standardized protocol should be adopted ( Box 2 ).