Prevalence of patients with congenital heart disease (CHD) is rapidly increasing due to continuous advancements in diagnostic techniques and medical or surgical treatment approaches. Along with cardiac computed tomography angiography, cardiac magnetic resonance (CMR) serves as a fundamental imaging modality for pre-surgical planning in patients with CHD, as CMR allows for the evaluation of cardiac and great vessel anatomy, biventricular function, flow dynamics, and tissue characterization. This information is essential for risk-assessment and optimal timing of surgical interventions. This article discusses the current role of pediatric cardiac MR imaging as a practical preoperative assessment tool in the pediatric population.
Key points
- •
Congenital heart disease can be routinely evaluated with cardiac magnetic resonance.
- •
Cardiac magnetic resonance provides information regarding biventricular function, flow, and tissue characterization.
- •
Cardiac magnetic resonance in pediatric patients can be helpful for surgical planning.
Introduction
The prevalence of congenital heart disease (CHD) is estimated to range around 4/1000 and 50/1000 among births in the United States. Over the last decade, continuous advancements in diagnostic and therapeutic techniques have led to an increased long-term survival of patients with CHD. Nowadays, the prevalence of adults with CHD is surpassing that of the pediatric population.
Several complications or sequelae may occur in adult patients with CHD who have undergone surgical intervention. Some cardiac abnormalities are common after the operation, and may require lifelong follow-ups. As children with CHD continue to grow, they may be more susceptible to experience distortion in post-surgical cardiovascular anatomy or modifications of biventricular volumes and function. These abnormalities may benefit from further palliative or corrective interventions in order to prevent the development of heart failure or cardiac arrhythmias. Therefore, multi-modality assessment of CHD is fundamental for anatomic and functional evaluation and optimal therapeutic planning. Echocardiography still represents the first line of imaging in patients with CHD because it is inexpensive and allows a reliable, non-invasive, real-time evaluation of cardiac and vascular anatomy, biventricular function, and valvular disease. However, its diagnostic value is often influenced by the limited acoustic windows. Invasive catheter angiography (ICA), another potential diagnostic modality, allows for the evaluation of vascular structures, blood flow-related parameters, and pressure. Furthermore, ICA can also be combined with therapeutic intervention in selected cases. The main disadvantages of ICA, however, are the invasive nature of the technique, the use of ionizing radiation, and its substantial operator dependence. The latter limitations led to the widespread use of non-invasive imaging modalities, such as cardiac computed tomography angiography, especially in patients who need shorter examinations focused on the evaluation of cardiac anatomy or function.
Although various computed tomography vendors have developed different strategies to reduce radiation dose, radiation and contrast exposure is still a concern when repeated studies are needed, especially in the pediatric population. Therefore, cardiac magnetic resonance (CMR) may represent an optimal non-invasive imaging technique that allows the evaluation of complex cardiac and extra-cardiac anatomy, biventricular function, flow dynamics, and tissue characterization without radiation exposure. It is important to note that CMR also has some limitations including the time-consuming image acquisition or the crucial need for patient compliance that may be challenging in small children without general anesthesia or sedation. However, high-quality images obtained with CMR provide invaluable support for diagnosis, prognostic stratification, and surgical planning in the CHD population.
MR Imaging Techniques
Younger pediatric patients with CHD are usually uncooperative and require a fast CMR acquisition preferably in a free-breathing fashion. To circumvent this issue, CMR may be performed under general anesthesia in selected pediatric patients, for example, children under 7 years of age; however, the recommendations in this regard are not in consensus.
Despite the wide range of CMR pulse sequences available in clinical practice, only few are routinely used for the evaluation of patients with CHD. The selection of the appropriate pulse sequences should be based on clinical indications. Cine images for the assessment of biventricular function, morphologic sequences for the visualization of anatomy, and phase-contrast velocity mapping acquisitions for the evaluation of pulmonary and systemic flow characteristics are fundamental for a complete CMR evaluation of patients with CHD. Additional pulse sequences, such as T2-weighted black blood sequences and T2* or T1 mapping, may be required in specific pathologies. The use of gadolinium-based contrast agents needs to be carefully managed, especially considering the potential for deposits that are observed in brain tissue after repeated administrations. Sequences typically used in pediatric CMR are shown in Fig. 1 . Clinical applications are summarized in Table 1 .

| Congenital Heart Diseases | CMR Pulse Sequences |
|---|---|
| Tetralogy of Fallot | Phase-contrast velocity mapping sequences Magnetic resonance angiography Cine images Late gadolinium enhancement T1 mapping |
| Congenitally corrected transposition of the great arteries | Phase-contrast velocity mapping sequences Cine images |
| Atrial septal defect | Phase-contrast velocity mapping sequences Cine images |
| Ventricular septal defect | Phase-contrast velocity mapping sequences Cine images |
| Anomalous pulmonary venous return | Phase-contrast velocity mapping sequences Cine images Magnetic resonance angiography |
| Aortic coarctation | Phase-contrast velocity mapping sequences Cine images Magnetic resonance angiography |
| Vascular rings | Cine images Black blood sequences Magnetic resonance angiography |
| Before and after Fontan correction | Cine images Magnetic resonance angiography Phase-contrast velocity mapping sequences |
Spin Echo Imaging
Black blood turbo spin echo (BBTSE) pulse sequences generate images with dark blood pool and variable signal intensity in the mediastinum structures based on the different tissue composition and weighting of the sequences. Acquisition of BBTSE in breath-hold along the axial, sagittal, and coronal planes allows for a reliable evaluation of the great vessels and cardiac anatomy. Compared with cine images, BBTSE sequences are not acquired through the whole cardiac cycle, but are timed in diastole or systole. Therefore, BBTSE acquisitions do not allow for the evaluation of segmental myocardial or global cardiac function, and are strictly confined to anatomic information. The main advantage of BBTSE is that these sequences are less susceptible to turbulent flow and metal-induced artifacts.
Electrocardiogram-Gated Cine Imaging
Electrocardiogram (ECG)-gated cine images are generally acquired using gradient echo cine pulse sequences resulting in bright blood signal. These sequences are usually performed with retrospective cardiac gating through the whole cardiac cycle and allow to generate multiple images in different cardiac phases that can be visualized in a cine loop. Prospective triggering is also available, which can be helpful in case of triggering problems or arrhythmias.
These cine images are most frequently acquired using standard spoiled gradient echo (SPGRE) or balanced steady-state free precession (bSSFP) pulse sequences.
Compared with SPGRE, bSSFP sequences are less sensitive to low-flow artifacts and allow for a faster acquisition and better discrimination between the blood pool and the myocardium. However, bSSFP sequences are more influenced by inconsistencies of the magnetic field, turbulent flow, and metal artifacts compared with SPGRE sequences. Retrospectively acquired multi-planar cine images allow for the assessment of the anatomy of the great vessels and qualitative evaluation of cardiac valve disease.
Furthermore, volumetric analysis of short axis or long axis cine images using dedicated software provides the evaluation of biventricular volumes and function.
In patients who cannot sustain breath-hold or with arrhythmias cine real-time images can represent a reasonable alternative for the evaluation of biventricular function and regional wall motion. In addition, real-time cine images have been investigated in the planning of interventional procedures.
Magnetic Resonance Angiography
Magnetic resonance angiography (MRA) allows for the evaluation of cardiovascular anatomy in patients with CHD. MRA acquisitions can be performed with or without the administration of a contrast agent. Contrast-enhanced MRA (CE-MRA), mainly acquired using 3D T1 SPGRE, requires the administration of a gadolinium-based contrast agent, with a usual dose of 0.1 to 0.2 mmol/kg. CE-MRA should be acquired during breath-hold in order to minimize motion artifacts in a relatively short acquisition time. Analysis of 2D or 3D CE-MRA datasets is usually performed with maximum intensity projection and volume-rendering reconstructions that are helpful for pre-surgical planning and post-operative evaluation. In particular, the relationship of mediastinal vessels in complex CHD can be visualized, providing supporting information for the physician to plan the optimal therapeutic approach.
Despite the fast acquisition using CE-MRA approaches, it is important to note that these techniques are not ECG gated, resulting in motion-blurring of the aortic root, coronary arteries, and cardiac chambers. Conversely, non-contrast MRAs (NCMRA), mostly based on 3D SSFP sequences, are generally ECG triggered. These pulse sequences can be acquired either in diastole or systole without the administration of a contrast agent. To prevent significant motion artifacts, NCMRAs are usually performed using a respiratory navigator. Although new sequences have been developed to shorten the acquisition time, the combination of respiratory and cardiac triggering can result in a longer scan time compared with CE-MRA. Considering that these sequences are acquired in a specific phase of the cardiac cycle, the evaluation of coronary artery anatomy becomes also possible. In addition, with NCMRA, the administration of gadolinium-based contrast agents can be avoided due to the high intrinsic signal and contrast-to-noise ratio between the blood pool and the surrounding cardiac or mediastinal structures.
Phase-Contrast Velocity Mapping Imaging
Phase-contrast velocity mapping pulse sequences allow for reliable flow quantification, velocity measurement, and evaluation of flow patterns in vessels. With the use of phase-contrast sequences, the ratio between pulmonary flow (Qp) and systemic flow (Qs) can be calculated (values of Qp/Qs < or >1 can be considered pathologic). These phase-contrast acquisitions are sensitive to the speed of flow, and the velocity-encoding parameters should be carefully selected to avoid aliasing artifacts. To prevent partial volume artifacts, slice thickness and slab orientation should be appropriately chosen. Images have to be positioned perpendicular to the vessel flow with the isocenter of acquisition positioned in the center of the vessel. Acquisitions can be performed during a single breath-hold or in free breathing using multiple averages. Retrospective ECG-gated acquisitions are preferred to prospective acquisitions because the former allows the evaluation of the whole diastole.
Late Gadolinium Enhancement
Late gadolinium enhancement (LGE) sequences are usually acquired 10 to 15 minutes after the injection of a gadolinium-based contrast agent. Although different types of LGE acquisitions are available in clinical practice, the most widely used are the T1-weighted inversion recovery sequences. The LGE images that such sequences provide show the signal intensity of the normal myocardium as nulled (black) and a hyperintense signal in the damaged areas. The latter represents the pathologic expression of decreased wash-out rate of the contrast agent caused by an increased extracellular volume (ECV). The inversion time has to be carefully chosen to obtain an optimal nulling of the normal myocardium. With the time elapsing after contrast administration, it is important to gradually increase the inversion time to adjust for the change in the contrast environment. Furthermore, using high spatial resolution is crucial for an optimal evaluation of the right ventricle (RV). Assessment of LGE in different CHD cases can be fundamental for the evaluation of arrhythmogenic substrates and for pre-surgical tissue characterization. Macroscopic fibrosis in patients with tetralogy of Fallot (TOF) can be related to the surgical procedure, but it can also be attributable to RV hypertrophy or secondary dilatation. In patients where the RV sustains the systemic circulation, the presence of myocardial LGE may predict arrhythmias, and progressive clinical deterioration.
T1 Mapping
Although the evaluation of replacement fibrosis can be detected with standard LGE, several limitations of that technique need to be considered. A misleading evaluation of LGE can result from unsuccessful nulling of the normal myocardium, field inhomogeneity, and the choice of quantification method. However, the T1 mapping approach is able to overcome the aforementioned issues. T1 mapping can provide data on tissue characterization without the administration of contrast agent. In addition, it allows for the evaluation of the change in ECV using the combination of native and post-contrast T1 mapping approaches. Different vendors have developed various pulse sequence schemes for T1 mapping that can be routinely adopted according to the clinical setting. For example, Broberg and colleagues showed that patients with repaired TOF (rTOF) have elevated ECV values compared with normal controls, and that patients with ECV greater than 30% had significantly higher percentage of clinical events. Increased ECV was also observed in patients with transposition of the great arteries who underwent arterial switch operations. Although there is still a debate surrounding the use of T1 mapping for the evaluation of CHD, the available evidence indicates that this approach will potentially play a key role in prognostic stratification.
Spectrum of imaging findings
Tetralogy of Fallot
Tetralogy of Fallot is the most common cyanotic CHD and is characterized by the malalignment of the infundibular septum. This anatomic defect causes an RV outflow tract (RVOT) obstruction, right ventricular hypertrophy, overriding aorta, and ventricular septal defect. The combination of these abnormalities may lead patients with TOF to develop different degrees of cyanosis.
The RVOT obstruction can range from mild, with normal pulmonary trunk and branches, to pulmonary atresia (PA), with severely hypoplastic pulmonary trunk and branches. In patients with TOF characterized by severe hypoplasia (or aplasia), the pulmonary circulation can be sustained by the development of major aortopulmonary collateral arteries. The major goal of early palliation in patients with TOF is the relief of the RVOT obstruction and closure of the ventricular septal defects (VSDs). Therefore, the pulmonary infundibulum is surgically opened typically by cutting through the annulus of the pulmonic valve. Subsequently, a patch is applied to augment the RVOT and/or the main pulmonary artery (hence: “transannular patch”). In addition, the ventricular septum defect is closed. After the surgery, the physiologic circulation is restored; however, pulmonic regurgitation is a common and essentially expected complication that in the long run leads to progressive RV dilatation, with associated diastolic and systolic dysfunction.
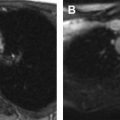
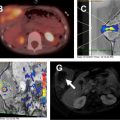
Preoperative evaluation later in life is crucial for establishing the correct timing of valve surgery in rTOF. Ultimately, the main goal is to restore valve competence with pulmonic valve replacement (PVR) and to achieve progressive reduction of RV dimensions by remodeling. Cardiac magnetic resonance has a key role in the accurate planning of PVR in patients with rTOF. Buechel and colleagues demonstrated that rTOF patients with end-diastolic volume (EDV) less than 150 mL/m 2 may benefit from PVR, with a chance to reduce RV dilatation. Frigiola and colleagues have identified a cut-off value for the EDV ratio between RV and left ventricle (LV) greater than 2 associated with an abnormal exercise test for the correct timing of PVR. In addition, a cut-off value of EDV approximately equal to 80 mL/m 2 is associated with a recovery of RV dimensions. Cine images are helpful in rTOF in the evaluation of residual VSDs and possible RVOT abnormalities, such as obstruction or aneurysm. Phase-contrast images acquired across the pulmonary artery provide information regarding regurgitation. Magnetic resonance angiography sequences can visualize stenosis in the pulmonary branches, as well as the presence of major aortopulmonary collateral arteries, among patients with rTOF. The presence of LGE in patients with rTOF has not been extensively investigated in the literature, and its clinical significance is doubtful. Park and colleagues showed that the extension of fibrosis is correlated with fragmented QRS complex. Although TOF is a pathology with predominantly right heart involvement, a few investigators showed increased values in native T1 and ECV in both ventricles, with findings more evident in girls than boys. The combination of data obtained by T1 mapping values, RV function and exercise tolerance may play a key role in terms of therapeutic approach in girls. Representative cases of TOF are shown in Figs. 2 and 3 .


Congenitally Corrected Transposition of the Great Arteries
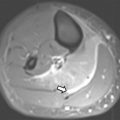
Levo-transposition of the great arteries (L-TGA), also called congenitally corrected TGA, is characterized by atrioventricular and ventriculoarterial discordance. Depending whether or not it is associated with other cardiac abnormalities, L-TGA may only be diagnosed in the adulthood. Although physiologic blood oxygenation is preserved in L-TGA patients, the RV sustains the systemic circulation; therefore, it is not uncommon to observe progressive RV dysfunction and tricuspid regurgitation over time. A surgical approach to correct this defect is not always recommended, but if it is clinically indicated then it is completed by a “double switch.” This operation is a combination of an atrial switch and either an arterial switch or a Rastelli procedure, which allows the anatomic restoration of the atrioventricular and ventriculoarterial connections. Preoperative evaluation of L-TGA includes an evaluation of biventricular volumes using cine images, with special focus on the RV. Tricuspid regurgitation can be quantified based on the combination of phase-contrast and cine acquisitions, that is, by subtracting the phase-contrast-based forward volume in the pulmonary artery from the cine-based volumetric RV stroke volume. A case of L-TGA is showed in Fig. 4 .

Atrial Septal Defects
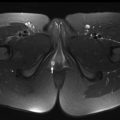
Atrial septal defects (ASDs) are mainly diagnosed in adulthood and have the potential to cause clinical manifestations such as arrhythmia, stroke, pulmonary embolism, or, in rare cases, pulmonary hypertension. There are several types of ASDs including the most common ostium secundum, and others such as ostium primum, unroofed coronary sinus, and sinus venosus defects. The latter types are uncommon, accounting for 3% to 10% of all ASDs. Sinus venosus defects can be located near the orifice of the superior vena cava (SVC) or inferior vena cava. If located near the SVC, the ASD is usually associated with anomalous pulmonary venous drainage in the right atrium or SVC. CMR evaluation of ASDs focuses on the visualization of anatomy and quantification of flows. Cine image stacks acquired in the axial plane are helpful for the evaluation of anatomy and assessment of partial anomalous pulmonary venous return (PAPVR). Short axis cine images provide information regarding RV dilatation. Considering that ASDs are pre-tricuspid shunts, a dilatation of the RV is generally observed. Phase-contrast sequences acquired across the pulmonary artery and the aorta are useful for a correct estimation of Qp/Qs. A Qp/Qs greater than 1.5 and dilatation of the right chambers indicate the need for surgical correction. MRA may be useful for the evaluation of PAPVR associated with sinus venosus ASDs. A representative case of a patient with ASDs is shown in Fig. 5 .

Ventricular Septal Defects
Accounting for greater than 20% of cardiac malformations, VSDs are the most common CHD in children. Among the several types of VSDs that have been described, the perimembranous VSD is the most common and clinically relevant, requiring surgical repair. Other types include muscular, inlet septum, outlet septum, and misalignment of the conal septum. Muscular defects if small do not usually require surgery. A left to right shunt occurs in systole; the severity of the shunt is correlated to the size of the VSD and pulmonary vascular resistance. Volume overload of the LV is commonly observed in patients with VSDs; which may progress to LV dilation, left atrial hypertension, and subsequently left heart failure over time. Preoperative CMR is useful for the evaluation of Qp/Qs measured using phase-contrast images positioned across the pulmonary artery and the ascending aorta. Cine image stacks acquired in short axis are useful for the evaluation of LV volumes. Complex cases of patients with VSDs are shown in Figs. 6–8 .