, Ella Yevdayev2, Aarti Kaushik3, 4 and Hollie A. Lai5
(1)
Long Beach Memorial Medical Center, Long Beach, CA, USA
(2)
Keck School of Medicine, University of Southern California, Los Angeles, CA, USA
(3)
Kaiser Permanente, Southern California Permanente Medical Group, Riverside, CA, USA
(4)
Molecular Imaging Center and PET Clinic, University of Southern California, Los Angeles, CA, USA
(5)
Department of Radiology and Nuclear Medicine, Children’s Hospital Los Angeles, Los Angeles, CA, USA
Case 14.1: Adrenal Cortical Cancer
History
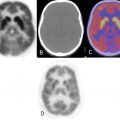
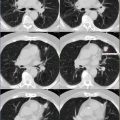
A 15-year-old female with known right adrenal cortical adenocarcinoma, status post chemotherapy treatment. PET/CT scan reported pulmonary metastases in the left lung and increase in size in the right adrenal mass.
Findings
Chest: There are two hypermetabolic left lung pulmonary lesions, one in the lateral lingual segment and second at the base (lower lobe), suggesting persistently active pulmonary metastases (measuring approximately 9–10 mm) (Fig. 14.1). The lingular segment nodule, SUV max 4.07. Left lung base nodule, SUV max of 4.07.
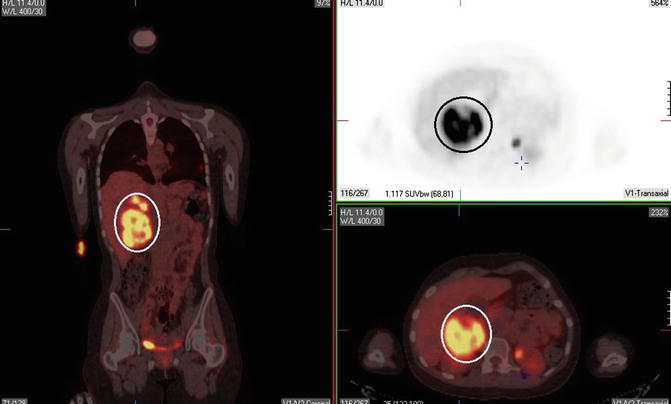
Fig. 14.1
Abdomen: A 8.0 × 4.5 × 10.8 cm right adrenal mass, SUV max 18.7 (Fig. 14.2). There are two separate focal areas of intensely increased FDG uptake superior to the mass, more medial, SUV max 18.7 and 12. 7 in the more lateral nodule. Suggestive for metastatic disease. There is noted subtle ill-defined hypoattenuating lesion in the liver seen on unenhanced CT, which demonstrates no significant corresponding FDG uptake on the PET. Lesions seen in the dome of the liver in segment 8 measure approximately 1.2 × 2.5 cm.
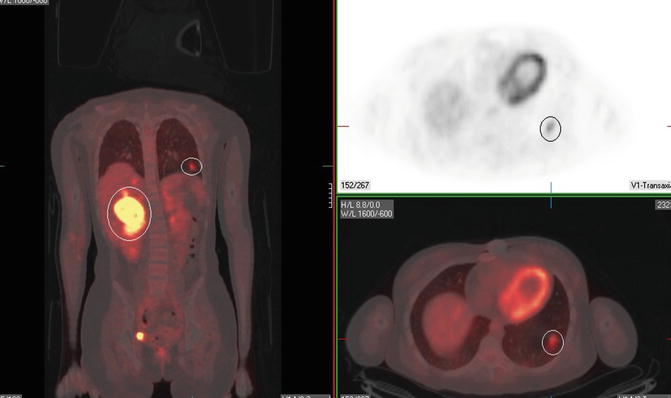
Fig. 14.2
Impression
PET/CT scan demonstrating hypermetabolic pulmonary nodules and right adrenal mass, suggestive for residual metabolically avid local and metastatic disease.
Pearls and Pitfalls
FDG PET for characterization of adrenal lesions showed a sensitivity of 100 %, a specificity of 94 %, and an accuracy of 96 %.
Discussion
Adrenal cortical carcinoma (ACC) is a rare malignant neoplasm with a poor prognosis.
FDG PET showed excellent diagnostic performance in differentiating adrenal lesions detected on CT or MRI. Because FDG PET has the additional advantage of evaluating the primary lesions as well as metastases, it could be cost-effective and the modality of staging. Most adrenocortical carcinomas accumulate and retain FDG and thus can be visualized by PET. However, false-negative findings are possible, especially with very small lesions.
Case 14.2: Thyroid Canc er: Recurrence
History
A 12-year-old female who was discovered to have a right thyroid lobe nodule on routine physical examination which ultimately turned out to be a T3, N1a, Mx papillary thyroid carcinoma. The patient is status post total thyroidectomy, after which she received 50 mCi of I-131. The patient presented with reportedly elevated thyroglobulin levels. Recent whole-body I-123 scan reported no definitive scintigraphic findings of iodine uptake to suggest a site of locally recurrent and/or metastatic disease.
Findings
Neck: A mildly FDG-avid 4 mm right lower cervical node focus of prominent FDG uptake is seen (SUV max 3.21) (Fig. 14.3). Two or three subtle focal areas of mildly increased FDG uptake are noted in the right lower neck on PET in the midst of the brown fat which appears to correspond to the very subtle subcentimeter-sized nodes on unenhanced CT (Fig. 14.4).
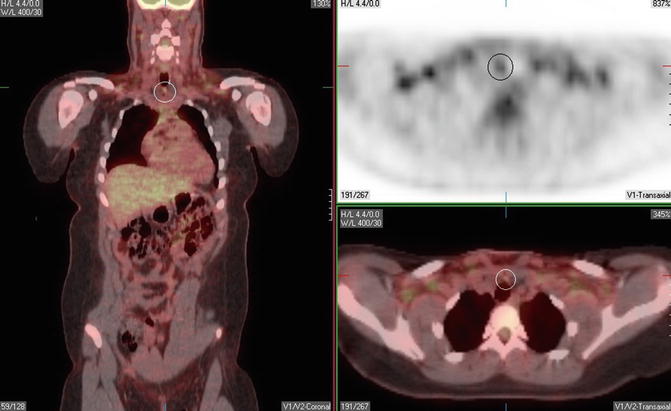
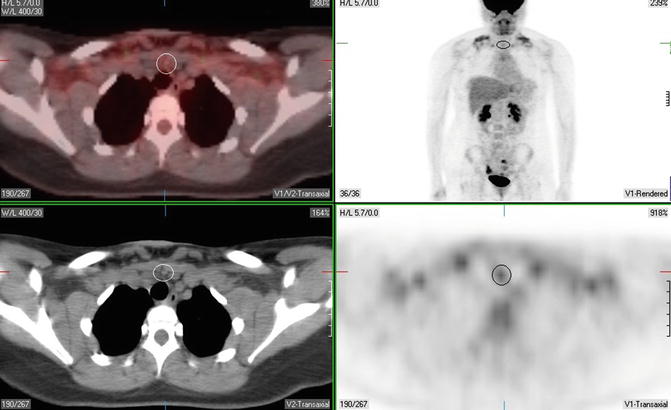
Fig. 14.3
Fig. 14.4
Impression
Restaging PET/CT scan demonstrating subtle subcentimeter-sized mildly FDG-avid nodes in the right lower neck, as detailed above. In the setting of reportedly elevated thyroglobulin levels, these questionable areas of uptake raise concern for possible sites of residual/recurrent disease.
Pearls and Pitfalls
1.
Only 50–60 % of papillary thyroid carcinomas and 64–70 % of follicular carcinomas are iodine avid.
2.
PET is not indicated for primary thyroid malignancy detection since FDG can accumulate in normal thyroid tissue (about 30 % of patients) and certain benign thyroid disease.
3.
A PET study will usually be positive in patients with thyroglobulin level higher than 100 μg/L. PET will detect true positive disease in 11 %, 50 %, and 90 % of patients with hTg levels of <10 μg/L, 10–20 μg/L, and >100 μg/L, respectively.
4.
FDG PET/CT is indicated for a known, differentiated, and recurrent papillary/follicular thyroid cancer patients with a negative I-131 scan. Increased expression of GLUT-1 is associated with the loss of radioactive iodine uptake in metastases.
Discussion
Less than 1 % of all cancer death are from thyroid cancer. FNA is best for accurate diagnosis for primary tumor. Coregistered 18F-FDG PET/CT can provide precise anatomic localization of recurrent or metastatic thyroid carcinoma, leading to improved diagnostic accuracy, and can guide therapeutic management. In addition, further assessment of 131I WBS-negative, thyroglobulin-positive patients by 18F-FDG PET/CT may aid in the clinical management of selected cases regardless of the thyroglobulin level (Figs. 14.3 and 14.4).
Case 14.3: Burkitt’s Lymphoma
History
A 15-year-old female with reported newly diagnosed Burkitt’s lymphoma.
Findings
There are prominent focal symmetric regions of intense FDG uptake bilaterally in the posterior triangle on the upper neck and bilateral supraclavicular regions, which demonstrate no corresponding anatomic correlate on unenhanced CT and likely represent brown fat activity (Fig. 14.5). Tiny, subcentimeter bilateral cervical nodes are seen in the midst of these areas of likely physiologic brown fat activity. There are symmetric regions of intense FDG uptake in the superior mediastinum and bilaterally in the axillae, which demonstrate no corresponding anatomic correlate on CT and also likely represent physiologic brown fat activity (Fig. 14.6). Bilateral symmetric paravertebral intense FDG uptake is seen along the entire thoracic spine, also without corresponding anatomic correlates on CT and also likely physiologic brown fat uptake.

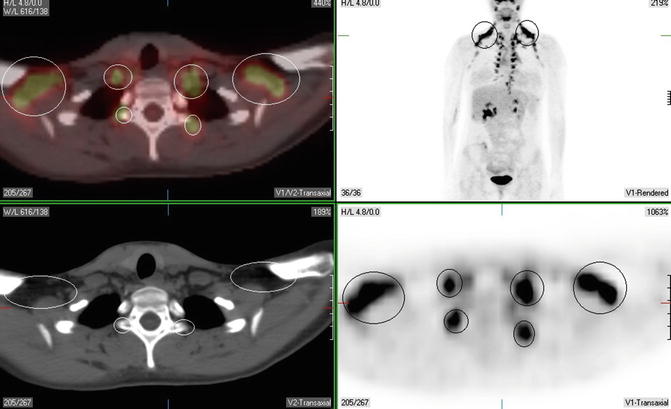
Fig. 14.5
Fig. 14.6
Impression
Prominent most symmetric likely physiologic brown fat activity is seen in bilateral upper neck, supraclavicular regions, superior mediastinum, and axillae. A few scattered subcentimeter nodes are seen in the midst of this brown fat uptake (especially in axillae), in which disease involvement cannot be entirely excluded as detailed above.
Pearls and Pitfalls
1.
Overall sensitivities, specificities, and positive and negative predictive values were 78 %, 98 %, 94 %, and 90 % for F-18 FDG PET and 79 %, 88 %, 90 %, and 46 % for CT, respectively.
2.
PET/CT scan with uptake greater than that of the liver is considered positive. Uptake that increased over the background but less than in the liver is equivocal.
3.
Coregistered PET/CT images significantly improve the specificity of PET findings. In this case, areas of significant focal FDG uptake in head/neck and chest demonstrate no correlates on CT, enabling differentiation between disease-involved nodes and physiologic brown fat activity.
Discussion
F-18 FDG PET imaging is a useful technique for the staging and follow-up of pediatric patients with lymphoma.
Case 14.4: Hodgkin’s Disease
History
A 10-year-old male recently diagnosed with Hodgkin’s disease from the left cervical node biopsy and post initiation chemotherapy. Study is performed for scintigraphic staging.
Findings
Head and Neck: Focal region of prominent FDG uptake in seen in the nasopharynx (Waldeyer’s ring) more prominent on the left, which corresponds to ill-defined soft tissue fullness on unenhanced CT, which likely represents disease-involved tissue (Fig. 14.7). There is large heterogeneous area of moderate to intense FDG accumulation involving the entire left neck on PET, corresponding to the coalesced-appearing conglomeration of numerous levels II–IV left-sided cervical nodes, which likely represent disease-involved lymphadenopathy. In aggregate, this conglomerate measures approximately 7.5 × 3.6 cm. Several mild to moderate FDG-avid right-sided cervical nodes are seen involving levels II–IV, the largest of these nodes measures approximately 1 × 1.4 cm.
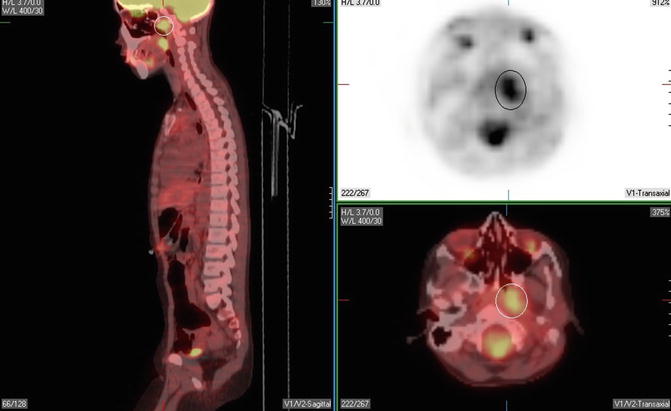
Fig. 14.7
Chest: Diffuse mild curvilinear FDG activity seen in the anterior mediastinum to the left of midline, which may represent reactive/rebound thymic tissue uptake. Left-sided Port-A-Cath seen in the left upper chest.
Abdomen: A focus of intense FDG uptake is seen in the upper anterior abdominal wall, which likely represents reactive uptake in the area of known G-tube (Fig. 14.8).
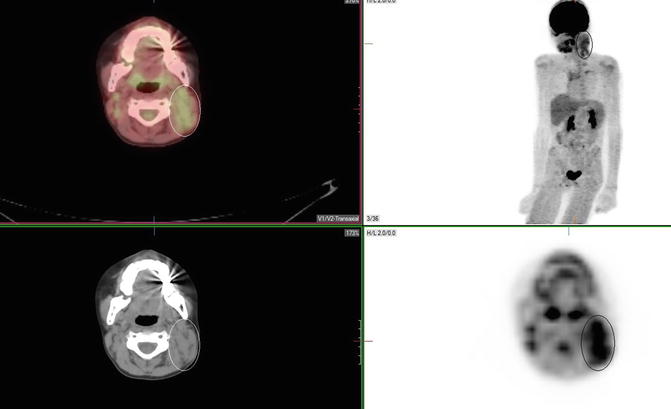
Fig. 14.8
Impression
PET/CT scan evidence for supradiaphragmatic hypermetabolic lymphadenopathy, predominantly in the Waldeyer’s ring and cervical nodes, left more than right, as detailed above.
Pearls and Pitfalls
1.
62–100 % of the FDG-positive patients will relapse after first-line chemotherapy; in contrast, only 4–16 % of the patients with negative PET will relapse.
2.
30–64 % of the residual masses will remain viable following the completion of therapy, demonstrating persistent metabolic uptake.
3.
Patient with a negative PET relapse in 16–25 % on a long-term follow-up.
4.
80 % of the patients who relapse do so at another nodal site.
Discussion
The prognosis for children and adolescents with Hodgkin’s lymphoma is excellent. However, many patients will show secondary malignancies 15–30 years after the initial diagnosis, which appears to be connected with the intensity of treatment during primary disease. The indication for radiotherapy in patients with early stage Hodgkin’s lymphoma should be further refined by using FDG PET for evaluating the response to chemotherapy. Furthermore, in patients at an advanced stage of the disease, it should be determined if sequential FDG PET research during chemotherapy can separate patients into subgroups with an excellent or a poor prognosis.
PET imaging plays an important role in staging, evaluating tumor response, planning radiation treatment fields, and monitoring after completion of therapy for pediatric Hodgkin’s lymphoma. This trend will likely increase in the future as a result of PET’s superior sensitivity in correlating sites of tumor activity compared to other available functional imaging modalities. Ongoing prospective studies of PET in pediatric patients will increase understanding about the optimal use of this modality in children with cancer and define the characteristics of FDG-avid nonmalignant conditions that may be problematic in the interpretation of tumor activity (Figs. 14.7 and 14.8).
Case 14.5: Rhabdomyosarcoma
History
A 7-month-old infant with reported left thigh rhabdomyosarcoma.
Findings
Chest: Diffuse mild curvilinear FDG activity seen in the anterior mediastinum to the left of midline, which may represent normal physiologic thymic tissue uptake in a 7-month-old infant.
Abdomen: Several moderately to intensely hypermetabolic, likely disease-involved periaortic nodes are seen on PET, the most cranial of which is seen at the level of L3, approximately measuring 0.8 cm (Fig. 14.9).
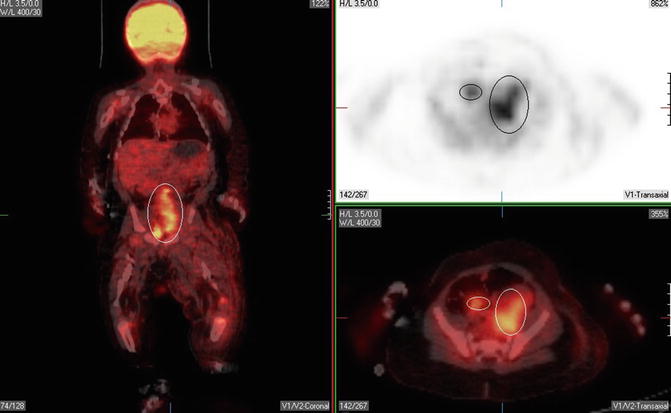
Fig. 14.9
Several adjacent focal regions of moderately intense FDG uptake are seen in the left pelvis/left groin (max SUV 3.69), which corresponds to a cystic appearing confluent mass with a thick periphery in the left pelvis on unenhanced CT, which likely represent bulky left iliac chain necrotic adenopathy, measuring 2.4 × 1.3 cm.
Several mildly to moderately hypermetabolic left-sided inguinal nodes, the largest of each measures 3 × 2.1 × 2.6 cm on unenhanced CT (Fig. 14.10).
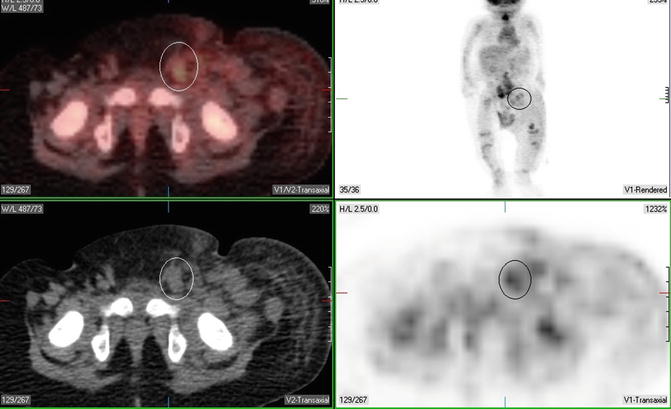
Fig. 14.10
A few scattered mostly subcentimeter right inguinal notes are also seen on unenhanced CT, which demonstrate mild corresponding FDG uptake on PET. Disease involvement cannot be excluded.
Edematous changes are seen in the subcutaneous tissue of the proximal left hip and thigh anteriorly along left thigh edema, likely a mass effect. Undescended right testicle is noted.
Musculoskeletal: Prominent focal region of intensely increased FDG uptake is seen in the posterior and lateral aspect of the left thigh (max SUV 4.87), corresponding to a heterogeneous appearing partially cystic/partially solid bilobed left thigh mass on unenhanced CT, with noted thickened walls and septations (Fig. 14.11). FDG uptake is mostly seen posteriorly in the solid component of this mass, while the more cystic/anterior regions of the mass demonstrate no abnormal FDG uptake.
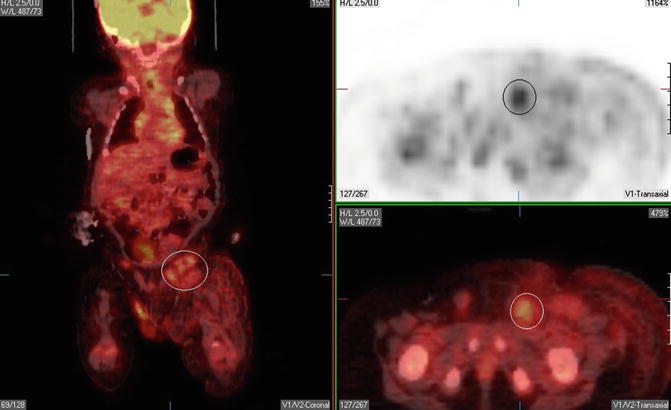
Fig. 14.11
Impression
1.
PET/CT scan demonstrates moderately hypermetabolic left thigh mass, which likely represents uptake in the site of the patient’s known rhabdomyosarcoma.
2.
Moderately to intensely hypermetabolic likely disease-involved periaortic, left iliac, and left inguinal bulky adenopathy, with questionable mildly FDG-avid subcentimeter right-sided inguinal nodes.
Pearls and Pitfalls
1.
High-grade sarcomas are generally more FDG-avid than low-grade lesions.
2.
Comparing PET with the final clinical determination of disease extent, PET is 77 % sensitive and 95 % specific.
Discussion
PET/CT useful in depicting an unknown primary rhabdomyosarcoma and detecting unsuspected and unusual metastatic sites of childhood sarcomas. It was useful in monitoring response to chemotherapy, radiation therapy, and radiofrequency ablation and aided the postoperative evaluation of tumor resection sites.
Case 14.6: Right Kidney Mass and History of Acute Lymphoid Leukemia
History
A 19-year-old female diagnosed with acute lymphoid leukemia as a child who has been in remission since treatment at that time. Recently, the patient reported right abdominal pain, and an abdominal CT reported a 2.8 cm × 2.3 cm × 2.3 cm heterogeneous hyperdense lesion which is partially exophytic in the right lower kidney.
Findings
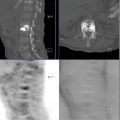
Abdomen/pelvis: Focal FDG uptake in a 2.8 × 2.3 × 2.3 cm heterogeneous hyperdense lesion in the right lower kidney pole (Fig. 14.12). The SUV max of this lesion is 3.04 on initial whole-body images, and 3.56 on post void delayed spot images of this region (Fig. 14.13). No FDG-avid abdominal and/or pelvic lymph nodes are seen.
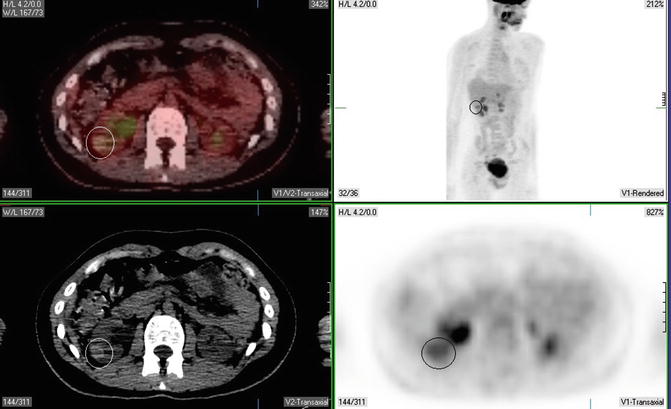
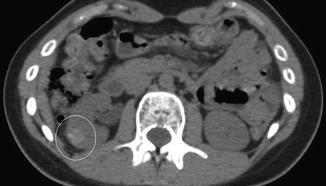
Fig. 14.12
Fig. 14.13
Impression
PET/CT scan demonstrating focal FDG uptake in the right lower kidney pole lesion, which persists on post void/post Lasix augmentation images. Findings raise concern for significant pathology.
Pearls and Pitfalls
FDG PET detected all the sites of distant metastasis revealed by CT, as well as additional metastatic sites, leading to an accuracy of 94 % vs. 89 % for CT. Although PET is more sensitive than CT for the characterization of renal masses, it lacks specificity given a background of physiologic tracer-labeled urine. As such, if we are able to “drive out” all physiologic tracer-labeled urine, we can significantly improve the specificity of PET/CT for these tumors. As such, our now standard acquisition protocol involves injection of 15–20 mg of Lasix IV 25–30 min post FDG administration. Additionally, the acquisition protocol also includes a single post void “bed” of the kidneys, as patient ambulation has proved valuable in allowing gravity to contribute to renal pelvis evacuation.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


