The last two and a half decades have seen phenomenal advances made in the field of cardiovascular magnetic resonance (CMR), and these advances have supported research into interventional applications using CMR. Conventional x-ray fluoroscopically guided cardiac catheterization and interventions are associated with the risk of exposure to ionizing radiation for both patients and staff. This is particularly relevant in younger patients, who are often required to undergo multiple procedures. The need for an imaging modality offering multiplanar imaging, superior structural delineation of complex cardiac anatomy, and additional physiologic information, without the risk of ionizing radiation, has brought CMR guidance of cardiac catheterization procedures to the fore. In the last 10 years, clinical programs using CMR-guided cardiac catheterization have developed and show promise.
Since the first magnetic resonance (MR) images showing live human anatomy were produced, this technique evolved to enable a variety of clinical applications of MR. Over the years, improvements in signal detection, fast data handling, advanced understanding of spin systems, pulse sequences, and artifact suppression have resulted in much faster scan times and considerable improvements in image resolution. These ultrafast imaging techniques form the basis of real-time imaging, used for CMR-guided cardiac catheterization. However, the first important step in making CMR cardiac catheterization a clinical reality is the design of a suitable interventional CMR system.
Interventional Cardiovascular Magnetic Resonance Systems
In the design of an interventional CMR suite, it is important to retain the full capabilities of a state-of-the-art diagnostic scanner without encumbering the interventionalist or creating a risk of high radiofrequency (RF) or switched magnetic field exposure. Open-magnet designs allow easier access to the patient, but are not typically available in field strengths higher than 1 T. The cylindrical horizontal bore systems offer higher field strengths and gradient slew rates, allowing higher-resolution imaging, shorter scan times, higher signal-to-noise ratio (SNR), reduced image distortion, and improved functionality with real-time imaging, all of which are of paramount importance when endovascular interventions are considered. A trade off with the traditional cylindrical magnet design is access to the patient. More recently, magnets with shorter bores and flared margins have been introduced and offer better patient access, especially for cardiovascular interventions, without compromising the advanced CMR features of diagnostic scanners. Rapid improvements in the processing power of computers, along with the use of powerful and intuitive software, have allowed researchers to develop novel strategies for image data acquisition and reconstruction. It is now possible to achieve frame rates of as high as 20 images per second with the aid of new parallel imaging techniques, while maintaining suitable spatial resolution for interventional applications.
Despite the inherent potential and promise of CMR-guided interventions and operations, there are still obstacles associated with performing the complete procedure in the CMR scanner, particularly because of the lack of CMR-compatible catheters and devices. Therefore the initial work in interventional CMR exploited multimodality imaging, such as x-ray and CMR (XMR) or XMR and ultrasound. Such hybrid units already in existence allow the use of separate modalities or a combination of them when needed. Cross-modality image integration, with spatial and temporal information about the anatomy, pathology, and therapy devices, can be provided to the users of these systems. XMR systems, which combine x-ray and CMR by having both modalities in the same room with a tabletop design, allow patients to be moved from one modality to the other in less than 1 minute ( Fig. 48.1 ).

Image fusion modalities are now in existence as a commercial product for clinical use. The use of x-ray fused with CMR (XFM) uses previously acquired CMR images and overlays them onto x-ray fluoroscopic images in the cardiac catheterization laboratory. These can be aligned by means of external fiduciary markers or internal anatomical structures, with the ability to correct for cardiac and respiratory motion. This has already been shown to reduce radiation exposure, screening time, and use of iodinated contrast agents in selected cases of cardiac catheterization in congenital heart disease. Although not a form of solely CMR-guided catheterization, such technology allows the application of CMR technology in the cardiac catheter laboratory even in nonhybrid suites.
Merits of Cardiovascular Magnetic Resonance Guidance
Improved Visualization of Cardiac Anatomy
A problem with x-ray-guided cardiac catheterization is the inherent poor contrast of soft tissues, such as the heart and great vessels. This makes it difficult for the cardiologist to manipulate or position guidewires, catheters, balloons, or interventional devices within the heart and surrounding vessels. A skilled operator usually relies on recognizing anatomic structures from previous experience or on contrast angiographic images acquired earlier in the procedure. The lack of adequate visualization increases the risk of perforating the heart or great vessels, especially when performing complex interventional procedures.
Certain interventional cardiac procedures involve selection of an appropriate cardiac device and its successful deployment within the heart, which requires accurate measurement of the size of defects and nearby anatomic structures. Such measurements are possible under x-ray fluoroscopy (XRF), but can be difficult.
A successful interventional cardiac procedure therefore relies heavily on adequate visualization of the heart or vessel. This implies the need for superior imaging methods that provide excellent visualization without increasing the risk to the patient. CMR fits this role very well because it provides exceptional structural delineation of both the heart and its surrounding vasculature and therefore allows safe guidance of interventional procedures.
Reduced Ionizing Radiation
There is a strong case for pediatric cardiac catheterization procedures to be made safer, especially in terms of ionizing radiation. According to the UK National Radiation Protection Board, the mean risk that a solid tumor will develop as a result of a single cardiac catheterization procedure is approximately 1 in 2500 in adults. This risk increases to 1 in 1000 in children if exposure occurs at 5 years of age. Also, the proportion of the body that is irradiated increases as the size of the patient decreases, and some procedures in patients with congenital heart disease often require much longer x-ray exposure. These risks are multiplied in children in particular, because they often undergo multiple cardiac catheter procedures. In addition to the patients, there is also a significant risk from ionizing radiation to the staff in the catheter laboratory during these procedures, despite the use of protective shields.
Physiologic Information
Conventional cardiac catheterization is used not only to provide anatomic information and perform intervention but also to obtain functional information. Invasive pressures and blood gases are commonly used to calculate systemic and pulmonary blood flow and resistance with the Fick principle. XRF angiography is also used to assess global ventricular function as well as regional wall motion abnormalities. The functional information obtained at cardiac catheterization is used alongside anatomic information to assess patient suitability for surgery or interventional cardiac catheterization or the need for long-term vasodilator therapy in patients with pulmonary vascular disease.
The Fick principle to quantify flow is dependent on multiple measurements (hemoglobin, aortic/pulmonary artery oxygen saturation, partial pressure, oxygen consumption), which can be a considerable source of inaccuracy. In addition, in patients with large intracardiac shunts and high pulmonary blood flow, accuracy is further reduced. Therefore there is a need for a method of flow quantification that allows accurate and reproducible measurement of pulmonary vascular resistance (PVR). Velocity encoded phase contrast CMR enables noninvasive quantification of blood flow in major vessels. Cardiac output and the pulmonary-to-systemic flow ratio (Qp:Qs) measured using this technique have been shown to be accurate. In addition, phase CMR has been validated in numerous phantom experiments, allowing for a novel method of quantification of PVR in patients with pulmonary hypertension by using invasive pressure measurements and CMR flow data. This method has since been used in a large clinical case series with good results and forms part of routine clinical practice in institutions where this is available.
Assessment of global and regional ventricular function can also be carried out much more accurately with cine steady-state free precession (SSFP) CMR than with x-ray angiography. When using CMR for assessing global ventricular function, there is no need to make assumptions about cardiac geometry, unlike with XRF or even echocardiography. This is particularly important when assessing right ventricular (RV) function and regional wall motion in the normal or systemic ventricle in patients with functionally single ventricle physiology.
Finally, combining invasive pressure measurements with CMR-derived blood flow and ventricular volumes also opens up interesting new ways of looking at pathophysiology. It allows for the study of pulmonary vascular compliance, derived ventricular pressure–volume loops, and assessment of load-independent ventricular function. Pharmacological stress studies have also been applied in CMR/XMR catheter studies to assess hemodynamic responses.
Magnetic Instrumentation and Visualization Strategies
Crucial to the success of interventional CMR is real-time tracking and visualization of catheters, guidewires, and devices in the CMR environment. Several groups around the world are putting considerable effort into developing CMR-suitable catheters and devices. Device localization under CMR is made possible by a variety of approaches that can be broadly classified as either electrically passive or electrically active.
Passive Catheter Tracking and Visualization
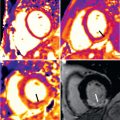
The passive tracking technique is commonly based on visualization of susceptibility artifacts or signal voids caused by the interventional device under CMR imaging. This is a well-studied technique and to date it is the most clinically feasible ( Figs. 48.2 and 48.3 ). Passive visualization often does not require any special hardware or software and therefore it can be performed on any commercial CMR system.


The ideal passive tracking catheter or guidewire must be made of a material that provides adequate physical properties such as torque and steerability, and allows tracking without obscuring the underlying anatomy. Ferromagnetic materials cause large susceptibility artifacts and therefore are not generally suitable for CMR-guided procedures. This rules out most metals used for making cardiac devices. However, certain alloys, such as nitinol (nickel and titanium), have magnetic susceptibility close to that of tissue. Therefore they are best suited for making guidewires and braided catheters that are MR compatible but not necessarily CMR safe.
The polymeric materials used for making catheters typically have low magnetic susceptibility and therefore cannot be easily localized on CMR images. This implies that, if materials with higher susceptibility can be incorporated into the wall of the catheters or sheaths or the lumen filled with a suitable contrast agent, then improved visualization can be achieved.
One approach to generating susceptibility artifacts is locally impregnating the catheter wall with gadolinium (Gd)-like compounds, such as dysprosium oxide, in the form of rings or along the length of the catheter during the extrusion process (see Fig. 48.2C ). Another approach is to use Gd contrast agents in varying concentrations within catheter lumens or impregnated into catheter walls to create either a positive or negative signal on CMR imaging.
Metallic devices and guidewires produce susceptibility artifacts, which aid visualization by way of the artifacts, but different metals behave differently under CMR. Titanium alloys produce narrower artifacts compared with ferromagnetic, or even certain other nonferromagnetic alloys such as nickel–chromium, which can produce large RF and susceptibility artifacts. However, commercial guidewires can heat up during CMR because of standing wave formation along the conductive parts longer than a quarter wavelength at the resonant frequency, which corresponds to approximately 12 cm in humans at 1.5 T, which is relevant for cardiac catheterization where wires are inserted to at least that length and nearly always much further.
Guidewires with a fiberglass core and nonmetallic guidewires made of resin microparticle compound covered by polytetrafluoroethylene have been used for MR-guided interventions in animals. More recent wire developments include the use of fiberglass MR safe guidewires, which were used in preclinical and clinical trials and led to successful interventions in congenital heart disease, but these were difficult to steer and proved to be fragile. There continues to be a drive for the development of an optimal guidewire and techniques to measure heating risks in vivo have been employed. Consequently, a newer nitinol based guidewire with iron oxide markers along the length to impart visibility has been developed with good preclinical results.
In the case of balloon angiographic catheters, if the balloon is inflated with carbon dioxide, as is done conventionally with x-ray, then the inflated balloon creates a signal void in the CMR image, thus enabling visualization (see Fig. 48.2A and B ). This method has been used successfully to guide catheters in patients under CMR (see Fig. 48.3 ). Although this technique allows easy visualization of the tip, the length is impossible to visualize because the signal void from the catheter length is masked by volume averaging and dephasing effects of thicker slices. A similar approach is to inflate the balloon of the angiographic catheter with a 1% concentration of Gd contrast agent and the balloon appears as a white ball because of the signal from the contrast-filled balloon.
The success of passive visualization also relies on dedicated scan techniques. A dynamic gradient echo sequence, such as SSFP, has been shown to be ideal for passive catheter tracking, especially when signal voids or susceptibility artifacts are used for visualization. Cardiac catheterization under XRF guidance is usually performed at imaging speeds of 25 to 30 frames per second. The frame rates available for CMR-guided interventions are not comparable because of the postprocessing of CMR images and their subsequent display, allowing a maximum of 10 to 14 frames routinely. Some of the proposed passive catheter tracking techniques require image subtraction or positive contrast to improve visualization of markers on the catheter, which means that, along with faster scan techniques, faster image processing algorithms are required.
Active Catheter Tracking and Visualization
The active catheter tracking and visualization method uses an electrical connection to the CMR scanner, and localization or tracking of the device requires the device itself, along with any additional hardware or software that comes with it. Typically, the device is equipped with a coil or an antenna that functions in either receive-only mode or transmit/receive mode.
Active catheters used as receivers have a coil or an antenna that receives signal from tissue in its immediate vicinity. These devices do not transmit signal into the patient but rely on the body coil to transmit into the patient. The signal received by these coils can then be used to pinpoint their position, for imaging of local tissue, or both. There are two important types of active catheters: those based on small coils positioned, for example, at the end of a catheter, and those based on a loopless antenna that can run along a catheter or can be made into a guidewire ( Fig. 48.4 ). In addition, active designs in which signal voids along the catheter are created by electrically controlled magnetic field inhomogeneities have also been investigated.

A small resonant coil at the tip of a catheter can be identified by a series of three one-dimensional (1D) projections along each axis. This can be done quickly (in three repetition times) and so could be repeated for very fast update of the catheter position, allowing real-time tracking of the catheter. The position of the catheter could then be projected over a previously acquired road map. Similar techniques have been combined with fast/real-time sequences, imaging the heart or vessels using surface coils, and the combined (interleaved) sequence has allowed simultaneous localization of the catheter and imaging of the surrounding tissue. Further adaptation of these sequences has allowed automatic changing of the imaging plane to match the change in the position of the catheter. Another development of active catheter tracking by the group at the National Institutes of Health allows the visualization of two simultaneously acquired planes as well as visualization of the catheter or device positions in real time, thus reducing the major problem of the catheter moving through the plane when only one imaging plane is visualized.
The great advantage of these active systems is that location of the catheter is unambiguous. Active visualization has great potential because it allows the whole length of the catheter or guidewire to be visualized and the imaging plane to be adapted to the moving catheter automatically. It may even allow high-resolution imaging of a small area of interest, such as a plaque in the vessel, when the coil or antenna is used in its imaging mode. However, the main disadvantage is concerned with safety. These devices use intravascular coils as RF antennas, and the connection to the external circuits via a long wire in the strong magnetic field makes induction of an electrical current and heating possible. There have been developments to overcome this risk, such as electrical decoupling of loopless antennas and the use of optical coupling and long fiber optic connections. An innovative active catheter design that uses miniaturized transformers showed no significant RF heating and holds promise for a safe transmission line for interventional applications ( Fig. 48.5 ).

Another approach to device localization is what some authors refer to as semiactive catheter tracking, implying passive localization of an electrically isolated resonant coil. These resonant coils locally enhance B 1 and signal reception so that, for very low global flip angles, the signal from the fiducial is prominent. The resonant coils can be interrogated by gradient echo sequences, such as SSFP with low flip angles. Catheters with multiple resonant coils can be tracked easily compared with passive catheters and have a relatively better safety profile compared with some of the active catheter designs ( Fig. 48.6 ).

Related posts:
 Use of Navigator Echoes in Cardiovascular Magnetic Resonance and Factors Affecting Their Implementation
Use of Navigator Echoes in Cardiovascular Magnetic Resonance and Factors Affecting Their Implementation
 Clinical Cardiovascular Magnetic Resonance Imaging Techniques
Clinical Cardiovascular Magnetic Resonance Imaging Techniques
 Atherosclerotic Plaque Imaging: Aorta and Carotid
Atherosclerotic Plaque Imaging: Aorta and Carotid
 T1 and T2 Mapping and Extracellular Volume in Cardiomyopathy
T1 and T2 Mapping and Extracellular Volume in Cardiomyopathy
 Cardiovascular Magnetic Resonance Assessment of Right Ventricular Anatomy and Function
Cardiovascular Magnetic Resonance Assessment of Right Ventricular Anatomy and Function
 Noncardiac Pathology
Noncardiac Pathology
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


