Appendicular skeleton
Humeri (AP)
Forearms (AP)
Hands (PA)
Femurs (AP)
Lower legs (AP)
Feet (AP)
Axial skeleton
Thorax (AP, lateral, right, and left obliques), to include ribs, thoracic, and upper lumbar spine
Pelvis (AP), to include the midlumbar spine
Lumbosacral spine (lateral)
Cervical spine (lateral)
Skull (frontal and lateral)
The skeletal survey should determine a level of specificity based on the nature, location, and chronicity of injury; however, no fracture in itself is pathognomic for child abuse. Fractures with high specificity of child abuse include rib fractures (especially posterior), classic metaphyseal lesions, scapular fractures, spinous process fractures, and sternal fractures. The classic metaphyseal lesions (Fig. 30.15a) are also known as corner or bucket-handle fractures, commonly caused by shearing force in manual assaults. Rib fractures are highly specific findings of abuse in cases of traumatic brain lesion, and they usually result from severe squeezing and shaking of the chest (Fig. 30.15b). Fractures with moderate specificity comprise multiple fractures, fractures of different ages, epiphyseal separations, vertebral body fractures and subluxations, digital fractures in nonambulatory children (Fig. 30.15c), and complex skull fractures. Common skeletal injuries with low specificity for child abuse consist of clavicular fractures (Fig. 30.15b), long bone shaft fractures, linear skull fractures, and subperiosteal new bone formation (Kleinman 1998; van Rijn and Sieswerda-Hoogendoorn 2012).
Metabolic bone disease such as rickets, skeletal dysplasia, osteogenesis imperfecta, and osteomyelitis can mimic child abuse. Thus, they should be excluded as a predisposing cause of multiple fractures.
30.3.8 Normal Anatomy and Variants Mimicking Trauma
Awareness of the normal developmental changes and variants in children is important, in order not to make errors in the interpretation of pediatric imaging. Irregularities of mineralization and secondary ossification centers are often confused with fracture. The ischiopubic synchondrosis can normally appear as asymmetric and bulky lesion, mimicking healing fracture (Fig. 30.16). Irregularity of distal femoral epiphysis is commonly observed on radiographs in children and is frequently bilateral, but not always symmetrical (Fig. 30.17). Normal physiologic periosteal new bone formation is most pronounced between 1 and 4 months, and most frequently involves femur, tibia, and humerus. Classic metaphyseal lesions which are seen in child abuse should be differentiated from normal metaphyseal variants including beaking or fragmentation (Kellenberger 2009; Keats and Anderson 2012).
Although most anatomic variants are asymptomatic, some variants such as os trigonum and os naviculare may be indeed clinically significant, causing pain (Lawson 1994). Thus, correlation with the radiographic findings and the clinical context is vital, and symptomatic variants can be further evaluated by bone scintigraphy or MRI.
30.4 Illustrations: Pediatric Skeletal Trauma
30.4.1 Incomplete Fracture

Fig. 30.1
Buckle fracture of the right distal radius in a 7-year-old girl with falling on outstretched hand. Right wrist radiograph shows a typical buckle fracture with outward buckling of the cortex (arrow)
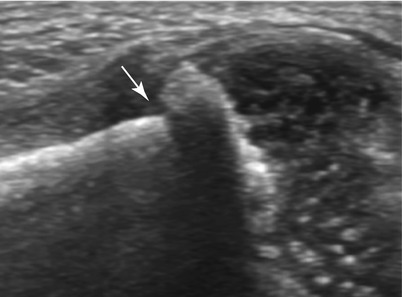
Fig. 30.2
Buckle fracture in a newborn boy who presented with irritability. Ultrasonography of the right humerus shows buckle fracture at the junction of metaphyseal and diaphyseal bone (arrow). The more porous metaphyseal bone fails in compression

Fig. 30.3
Greenstick fracture in a 4-year-old girl who fell off a bike. Lateral radiograph shows greenstick fracture on the convex side of the radius (arrow) and buckle fracture on the concave side of ulna (arrowhead)
30.4.2 Toddler’s Fracture

Fig. 30.4
Toddler’s fracture in a 3-year-old boy. Radiograph of the left lower leg shows spiral, nondisplaced fractures (arrows) through the distal tibia
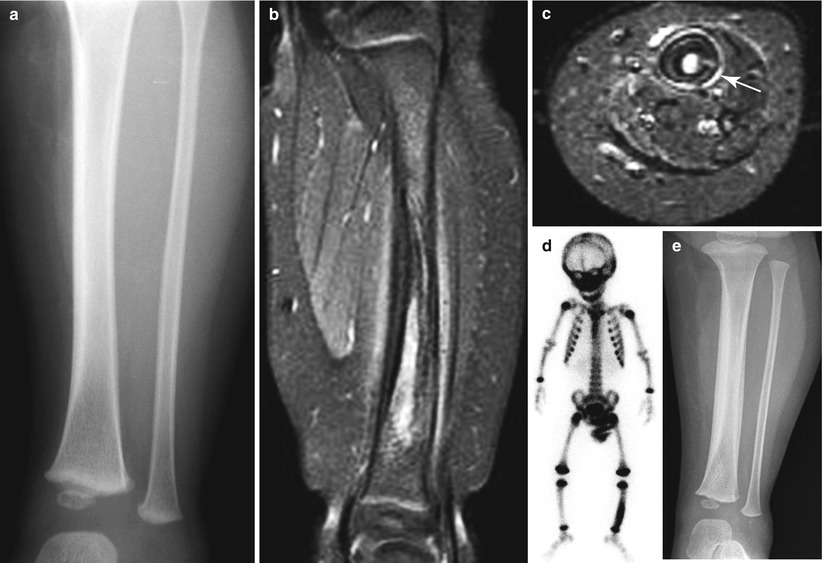
Fig. 30.5
Toddler’s fracture in a 2-year-old boy presented with limping gait. (a) Initial radiograph of left lower leg shows no bony abnormalities. (b, c) Fat-suppressed contrast-enhanced T1-weighted sagittal (b) and axial (c) MR images show fracture line (arrow in c) with surrounding marrow edema and periosteal reaction. (d) Bone scan shows increased uptake in the left tibia shaft. (e) Follow-up radiograph after 2 weeks reveals cortical thickening with periosteal reaction of the tibia (Courtesy of Dr. Lee HJ, Keimyung University School of Medicine)
30.4.3 Physeal Injury
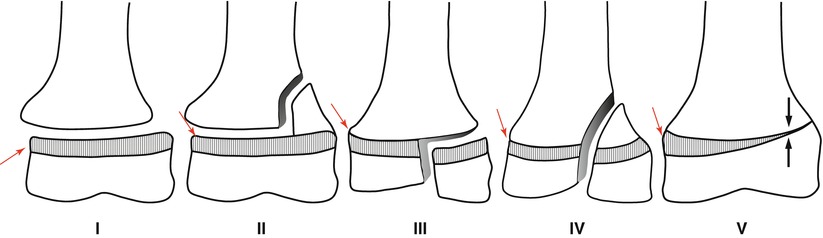
Fig. 30.6
Illustrations of the Salter-Harris classification of physeal injuries (see text)
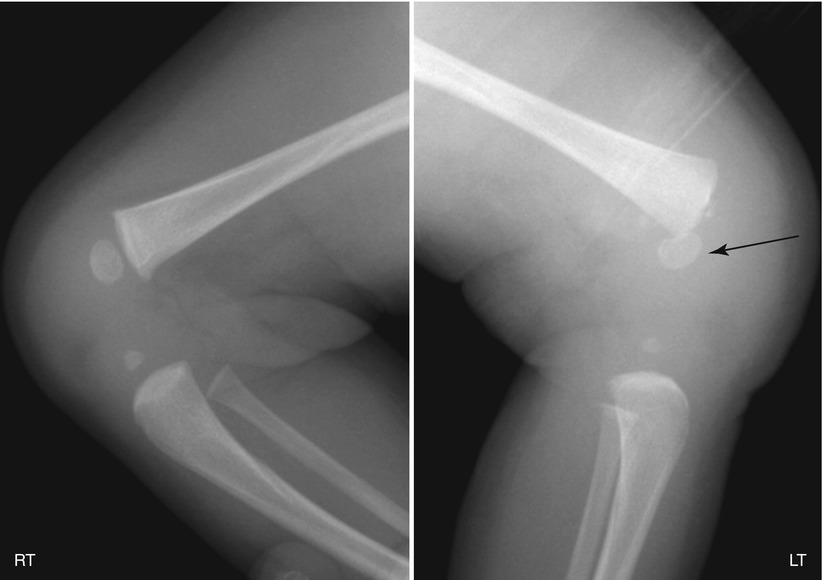
Fig. 30.7
Salter-Harris type 1 fracture in a newborn baby. Lateral radiographs of the knee show a complete posterior slip of epiphysis of the left distal femur (arrow) due to a fracture through the physis (Courtesy of Dr. Kim IO, Seoul National University Children’s Hospital)
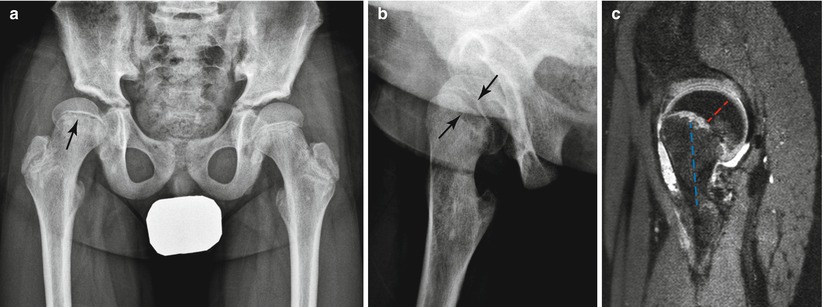
Fig. 30.8
Slipped capital femoral epiphysis, which is an example of Salter-Harris type 1 fracture, in a 12-year-old boy with hip pain. (a, b) Anteroposterior with neutral position and oblique radiographs show asymmetric widening of the physis of the right proximal femur (arrows). (c) 3D VISTA sagittal MR image depicts posterior rotation of the femoral epiphysis (red dotted line) relative to the metaphysis (blue dotted line), indicating retroversion at the epiphyseal–metaphyseal junction

Fig. 30.9
Salter-Harris type 2 fracture in an 11-year-old girl who had sustained a fall from height and injured her right ankle. (a, b) Anteroposterior radiograph and coronal CT image of the right ankle show a displaced metaphyseal fracture (arrow) and an extension into the physis (arrowhead) with a fibular shaft fracture by an abduction injury. (c) Proton density coronal MR image also demonstrates Salter-Harris type 2 fracture involving right ankle with soft tissue swelling and effusion
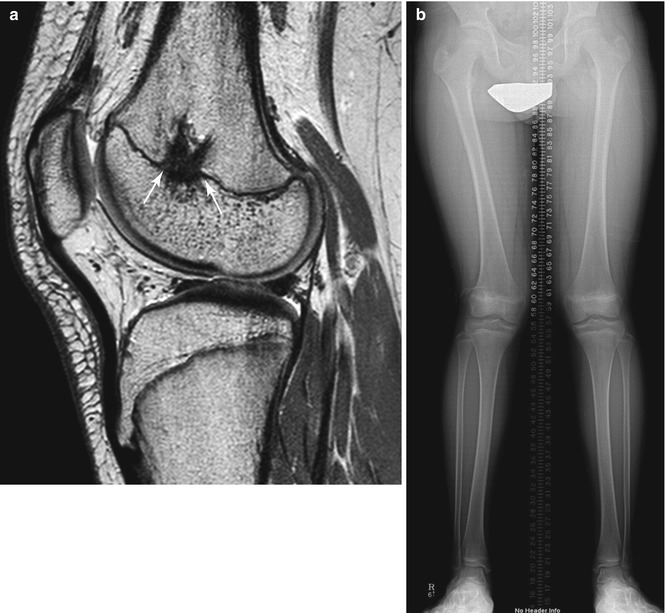
Fig. 30.10




Premature physeal closure in a 13-year-old boy after Salter-Harris type 2 fracture. (a) Sagittal proton density MR image shows a bony bridge (arrows) along the central, lateral aspect of the right distal femoral physis. (b) Anteroposterior radiograph of lower extremities shows a right valgus deformity with limb shortening
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
