Inflammatory and infectious disorders of the spine in children are less common than in adults, and are usually categorized according to location into (1) those predominantly affecting the spinal cord; (2) those predominantly affecting the nerve roots and meninges; and (3) those predominantly affecting the vertebrae, discs, and epidural space. Disorders primitively involving the spinal cord may be grouped into 2 basic categories: (1) inflammatory (represented by acute transverse myelopathy) and (2) infectious (ie, bacterial, viral, fungal, or parasitic). Inflammatory spinal cord diseases are more common than primitive spinal cord infection.
Key points
- •
Inflammatory and infectious disorders of the spine in children are less common than in adults, and are usually categorized according to location into (1) those predominantly affecting the spinal cord; (2) those predominantly affecting the nerve roots and meninges; and (3) those predominantly affecting the vertebrae, discs, and epidural space.
- •
Magnetic resonance (MR) imaging is the main imaging modality for diagnosing infectious and inflammatory disorders of the spine in the pediatric age group.
- •
Because of the often aspecific clinical presentation that may raise the suspicion of spinal cord compression, MR imaging is often performed in emergencies.
- •
Intravenous administration of contrast material (ie, gadolinium chelate) is of paramount importance for an adequate identification and characterization of these disorders.
Introduction
Inflammatory and infectious disorders of the spine in children are less common than in adults, and are usually categorized according to location into (1) those predominantly affecting the spinal cord; (2) those predominantly affecting the nerve roots and meninges; and (3) those predominantly affecting the vertebrae, discs, and epidural space.
Disorders predominantly affecting the spinal cord
Disorders primitively involving the spinal cord may be grouped into 2 basic categories: (1) inflammatory disorders, represented by acute transverse myelopathy; and (2) infectious disorders, which may be bacterial, viral, fungal, or parasitic. Inflammatory spinal cord diseases are much more common than primitive spinal cord infection.
Acute Transverse Myelopathy
Acute transverse myelopathy (ATM) is a focal inflammatory disorder of the spinal cord resulting in motor, sensory, and autonomic dysfunction. Individuals of all ages may be affected, with bimodal peaks between the ages of 10 and 19 years and 30 and 39 years. Although the terms ATM and acute transverse myelitis have often been used interchangeably, the former is a broad header that includes idiopathic forms (corresponding with acute transverse myelitis) and forms with known cause, such as postinfectious/postvaccination (ie, acute disseminated encephalomyelitis [ADEM]); neuromyelitis optica; multiple sclerosis; and ischemic, paraneoplastic, autoimmune, and postirradiation myelitis.
Idiopathic Acute Transverse Myelopathy
Clinical presentation is with pain, paresthesias, leg weakness, and sphincteral dysfunction, all of which progress to nadir between 4 hours and 21 days (usually 24 hours) following the onset of symptoms. It is thought that strokelike evolution (ie, nadir reached earlier than 4 hours) indicates vascular causes (spinal cord infarction). Signs and/or symptoms are usually bilateral, although not necessarily symmetric, and there usually is a clearly defined sensory level. Cerebrospinal fluid (CSF) analysis reveals signs of spinal cord inflammation, such as pleocytosis or increased immunoglobulin G (IgG) index.
The diagnosis of idiopathic ATM is one of exclusion, and involves 3 consecutive steps :
- 1.
Rule out a compressive cause: this requires contrast-enhanced magnetic resonance (MR) imaging of the entire spinal cord; if cord compression is ruled out and MR imaging indicates primary spinal cord involvement, MR imaging of the brain should also be performed;
- 2.
Define presence or absence of spinal cord inflammation by performing lumbar puncture with CSF analysis;
- 3.
Define extent of demyelination: brain MR imaging is analyzed for signs of involvement of the white matter and optic nerves. If none is found, idiopathic ATM is likely. If the white matter is involved, ADEM or multiple sclerosis should be considered. In addition, if the optic nerves are the only involved structure, neuromyelitis optica is likely. Visual evoked potentials are a significant diagnostic adjunct.
MR imaging criteria for myelitis ( Fig. 1 ) include normal or slightly expanded spinal cord showing diffuse or patchy hyperintensity on T2-weighted images, usually involving more than 1 vertebral level in length. There may be patchy enhancement after gadolinium administration. The conus medullaris is involved most frequently.
Prognosis of idiopathic ATM is variable, with one-third of patients recovering with little to no sequelae, one-third left with moderate degrees of permanent disability, and one-third having severe disabilities. Rapid progression of signs and symptoms at presentation usually portends a poor prognosis.
Acute Disseminated Encephalomyelitis
ADEM has been associated with viral infections (ie, postinfectious myelitis), such as measles, rubella, chickenpox, mumps, influenza, Epstein-Barr virus, Coxsackie B, cytomegalovirus, herpes simplex virus, hepatitis A virus, and adenoviruses, as well as with Borrelia , Mycoplasma pneumoniae , and nonspecific infection of the upper respiratory tract. Moreover, ADEM may also occur after vaccination (ie, postvaccination myelitis), including polio, rabies, smallpox, influenza, rubella, and plasma-derived form of hepatitis B. In most patients, postvaccination myelitis is a presumptive diagnosis based on the temporal relationship between vaccine administration and onset of symptoms.
Unlike idiopathic ATM, ADEM typically is characterized by extensive involvement of the brain. About 40% of patients with ADEM also show lesions in their spinal cords. The process usually is monophasic (ie, it occurs once in the life of the patient). However, multifocal disseminated encephalomyelitis has also been documented.
The disorder commonly begins 1 to 2 weeks after a viral, and seemingly minor, illness. The initial illness is often subclinical. Once the symptoms are present, they become more obvious 1 to 2 days after the diagnosis but may progress for up to 2 weeks. CSF analysis may show increased proteins and leukocytosis. The thoracic spinal cord is involved more often than the cervical region. On histology, there is necrosis and inflammation; perivascular lymphocytic infiltration and demyelination also are present.
On MR imaging, T2-weighted images may show multiple, more or less well-defined areas of increased signal intensity within the cord ( Fig. 2 ). Holocord involvement is possible. Segmental disease generally involves 2 to 3 vertebral bodies in length, and may expand the cord slightly. In ADEM, generally there is no enhancement after gadolinium administration, whereas enhancement is common in idiopathic ATM. In the latter condition, enhancement of the cauda equina may also be seen, suggesting that transverse myelitis and Guillain-Barré syndrome (GBS) may have a similar cause.
Multiple Sclerosis
Multiple sclerosis (MS) is rare in children, and spinal cord involvement is even rarer. Spinal cord plaques occur preferentially in the dorsolateral cord, and may be found at any segment. A predilection for the cervical segment has been reported in the early stages of the disease.
The MR imaging findings in childhood and juvenile MS mimic those of adult-onset MS. T2-weighted images show 1 or more elongated, poorly marginated, hyperintense intramedullary lesions. Acute demyelinating lesions may display mass effect and enhance after gadolinium administration ( Fig. 3 ).
Tumefactive plaques in the spinal cord have been reported in association with swelling and MR signal changes mimicking a neoplasm.
Neuromyelitis Optica
Neuromyelitis optica (NMO), formerly known as Devic disease, is a rare, severe, monophasic or multiphasic demyelinating disease of the central nervous system (CNS) that preferentially affects the optic nerves and spinal cord. The revised diagnostic criteria for NMO require the presence of optic neuritis and acute myelitis, associated with either a spinal MR imaging lesion extending over 3 or more segments, or positive NMO serology. It has been shown that presence of at least 2 of the following 3 laboratory findings is 99% sensitive and 90% specific for NMO: (1) contiguous spinal cord MR imaging lesion extending over more than 3 vertebral segments, (2) brain MR imaging not meeting criteria for MS, and (3) NMO-IgG seropositive status. NMO-IgG is an autoantibody found in the serum of patients affected by NMO, with 91% to 100% specificity and 75% to 90% sensitivity. NMO-IgG binds to aquaporin-4 (AQP4), which is the main channel that regulates water homeostasis in the CNS, mainly located around cerebral microvessels, pia mater, and Virchow-Robin sheaths.
Most affected patients are female, with a 9:1 gender predilection compared with male patients. Although mostly a disease of adults, NMO occasionally is seen in children. Typically, optic neuritis is severe, painful, unilateral rather than bilateral, and not simultaneous with ATM. Attacks of optic neuritis precede ATM in 80% of cases (usually <3 months), whereas ATM precedes optic neuritis in 20% of cases. Clinical findings in patients with myelitis prominently include severe symmetric paraplegia, sensory loss below the lesion, and bladder dysfunction. Atypical forms of NMO have recently been identified in which NMO-IgG seropositivity is found in patients with isolated longitudinally extensive transverse myelitis (LETM), monophasic or recurrent isolated optic neuritis, and brainstem encephalitis. The terms NMO spectrum disorder and autoimmune AQP4 channelopathy describe this host of conditions that encompass a larger group of patients than the classic NMO criteria.
Imaging of the entire craniospinal axis should always be performed in patients suspected of having NMO. Spinal MR imaging ( Fig. 4 ) typically shows LETM, characterized by large, confluent areas of high T2 signal intensity involving the spinal cord extensively. These lesions are typically longer than 3 vertebral bodies in a craniocaudal direction; they occasionally involve the entire span of the cord, and may enhance with gadolinium administration. The cord may be expanded and may show cavitation. Brain imaging of patients with suspected NMO shows optic nerve and chiasm involvement, characterized by swelling, T2-hyperintensity, and contrast enhancement in the acute demyelination phase. Although the brain may be unaffected, hypothalamic, periaqueductal gray, and area postrema lesions can be found in the context of NMO in up to 60% of cases in some studies.
Spinal cord infections
Spinal Cord Abscess/Granuloma
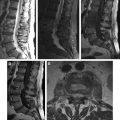
Bacterial spinal cord abscesses are extremely rare. Children account for up 20% to 50% of cases in some series. Among causative organisms, Schistosoma is particularly common in children. Tuberculosis is also gaining new ground in Western countries. Fungal diseases include candida infection, aspergillus, and nocardiosis. Predisposing conditions include congenital heart disease, disorders of the immune system, patients with long-term intravascular access lines, underlying spinal cord tumors, and dermal sinuses. Dermal sinuses may give rise to intraspinal abscesses outside and inside the spinal cord. Most patients have a history of infection elsewhere and spinal cord involvement may be secondary to either hematogenous or lymphatic spread. The process begins as a myelitis and, if left untreated, may progress to frank abscess formation.
MR imaging shows increased T2 signal intensity and expansion of the cord. A thin hypointense stripe surrounding the lesion indicates a capsule. After contrast administration there is ill-defined or well-defined marginal enhancement according to the stage of the inflammatory process ( Figs. 5 and 6 ). After initiation of treatment, the signal on T2-weighted images decreases and ring enhancement becomes prominent. With adequate therapy, the enhancement slowly resolves.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


