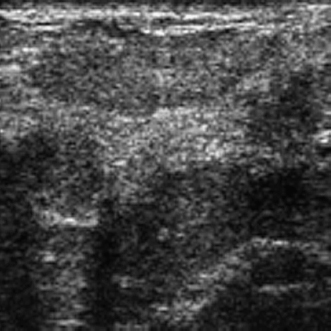
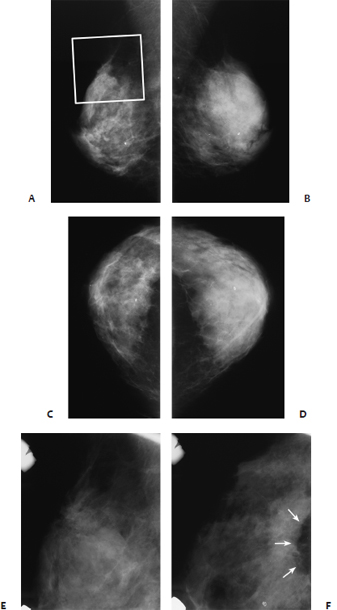
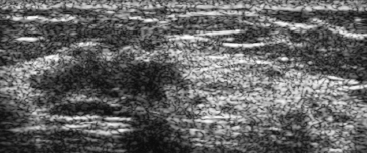
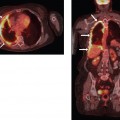
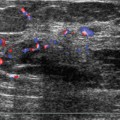
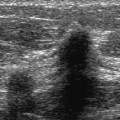
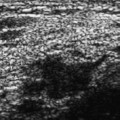
22 Peripheral Architectural Distortion A 62-year-old woman presents for screening mammogram. • Normal exam • Architectural distortion (Fig. 22.1) Fig. 22.1 In the right inferior inner breast, there is an area of architectural distortion (square). (A) Right MLO mammogram. (B) Left MLO mammogram. (C) Right CC mammogram. (D) Left CC mammogram. (E) Right MLO spot compression mammogram. Frequency • 13 MHz (Fig. 22.2) Fig. 22.2 Right antiradial breast sonogram. No sonographic mass is identified in the area of the mammographic architectural distortion. Only normal hyperechoic tissue is present. Fig. 22.3 Right sagittal dynamic bolus three-dimensional (3D) volume-gradient series breast MRI. In the area of the mammographic architectural distortion, MRI also demonstrates architectural distortion and skin thickening (square). However, there is no associated contrast enhancement of the area. Although MRI demonstrates architectural distortion and skin thickening, the lack of contrast enhancement suggests that the architectural distortion is benign. • Fibroadenomatoid hyperplasia • BI-RADS assessment category 4, suspicious; biopsy should be considered. • This case illustrates peripheral architectural distortion. The spot compression emphasizes the retraction of the edge of the parenchyma associated with abnormal deviation of the parenchymal lines. Normally, the axis of the parenchymal lines should be toward the nipple. In this case, they are pointing toward the skin away from the nipple. • The etiologies of architectural distortion are similar to the causes of irregular masses. Benign entities include scar, mastitis, fibrocystic changes, adenosis, mesenchymal lesions (fat necrosis, fibromatosis), and benign neoplasms (e.g., sclerosing papillomas, myofibroblastomas). Malignant entities include infiltrating ductal, invasive lobular, tubular, and occasionally lymphoma. Jones MK. Atlas of Breast Imaging. Malden, MA: Blackwell Science; 1996:108–112 A 54-year-old woman presents for screening mammogram. • Normal exam • Architectural distortion (Fig. 22.4) Fig. 22.4 There is architectural distortion of the superior edge of the right breast on the MLO view (square in A). Posterior parenchymal retraction is present on the right XCCL spot magnification view (arrows in F). (A) Right MLO mammogram. (B) Left MLO mammogram. (C) Right CC mammogram. (D) Left CC mammogram. (E) Right MLO spot magnification mammogram. (F) Right XCCL spot magnification mammogram. Frequency • 10 MHz Mass (Fig. 22.5) • Margin: ill defined • Echogenicity: hypoechoic • Retrotumoral acoustic appearance: single edge shadowing • Shape: irregular Fig. 22.5 Right radial breast sonogram. In the upper outer quadrant, the mammographic architectural distortion corresponds to an irregular hypoechoic mass. • Radial sclerosing lesion (radial scar) • Ductal carcinoma in situ • 0.8 cm ductal carcinoma in situ within the 2.2 cm radial scar • BI-RADS assessment category 4, suspicious; biopsy should be considered. • This case illustrates two common areas of architectural distortion in denser breasts: parenchymal retraction of the superior and posterior parenchymal edges. The superior edges of the breast should generally be symmetric in configuration. If there is asymmetry, the superior edge should have a curved or lobulated contour. The parenchymal density should gradually decrease until it blends into the axilla. When a mass produces parenchymal retraction, the superior edge loses the curved or lobular contour and forms a sharp triangular appearance. There is a greater difference between the density of the parenchymal edge and the axillary fat on the abnormal side compared with the normal side. • When a mass causes retraction of the posterior edge of the breast, the abnormal density forms a V and is termed the “tent” sign. Tabar L, Dean PB. Teaching Atlas of Mammography. 3rd ed. New York: Thieme; 2001:12–13, 119, 137 A 78-year-old woman presents for screening mammogram. Mass (Fig. 22.6) • Margin: spiculated • Shape: irregular
Case 22.1: Benign Process
Case History
Physical Examination
Mammogram

Ultrasound
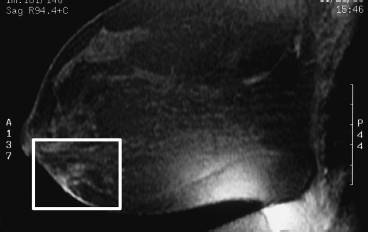
Other Modalities: MRI (Fig. 22.3)
MRI Findings
Pathology
Management
Pearls and Pitfalls
Suggested Reading
Case 22.2: Radial Scar
Case History
Physical Examination
Mammogram
Ultrasound
Pathology
Management
Pearls and Pitfalls
Suggested Reading
Case 22.3: Infiltrating Ductal Cancer
Case History
Mammogram
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


