Chapter Outline
The pharynx is the crossroads of respiration, speech, and swallowing. During respiration, the pharynx is an active conduit for the passage of air from the nasopharynx to the laryngeal aditus. During speech, the pharynx functions as a resonating chamber, changing size and shape to alter sounds. During swallowing, the pharynx directs the bolus into the esophagus and prevents the bolus from entering the tracheobronchial tree. Disorders of the pharynx may therefore be manifested by respiratory, speech, or swallowing dysfunction. Patients may complain of dysphagia, odynophagia, choking, or a feeling of a lump in the throat not associated with swallowing (a globus sensation). Soft palate insufficiency may be suggested by nasal regurgitation or a nasal voice quality. Recurrent pneumonia, asthma, chronic bronchitis, or coughing may indicate pharyngeal dysfunction. In this chapter, the focus is on the anatomy of the pharynx as a basis for understanding structural and motility disorders. The neurologic anatomy necessary for understanding motility disorders is presented in Chapter 15 .
Anatomy
Location
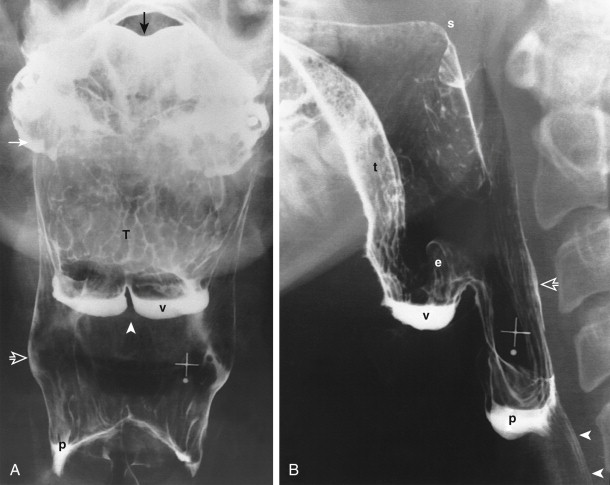
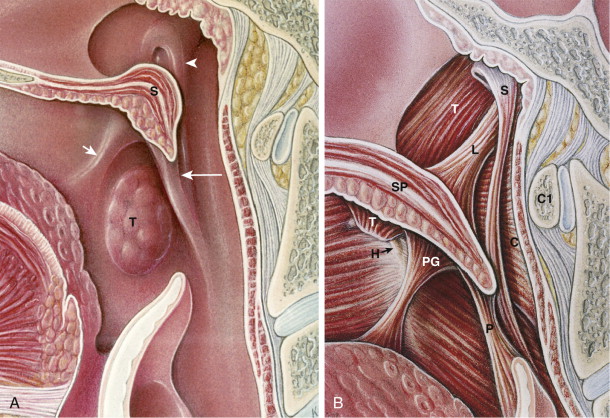
The pharynx is a funnel-shaped tube of skeletal muscle extending from the cranial base to the lower margin of the cricoid cartilage ( Fig. 14-1 ). The pharynx lies anterior to the vertebral bodies of the cervical spine, prevertebral muscles, and loose connective tissue of the retropharyngeal space. The pharynx is confined laterally by the muscles of the neck, lateral portions of the hyoid bone and thyroid cartilage, and carotid sheath ( Fig. 14-2 ). The pharynx and larynx are intimately related ( Fig 14-3 ), in embryologic origin and anatomically. The epiglottis and remainder of the supraglottis are of pharyngeal, not laryngeal origin.

Basic Structures and Mucosal Surface Patterns
The shape of the pharynx is determined by the underlying musculature, laryngeal cartilages, and supporting skeleton. Although the nasopharynx is primarily a respiratory tract structure, certain nasopharyngeal structures participate in the act of swallowing. The eustachian tube connects the middle ear with the nasopharynx, allowing equilibration of air pressures on the internal and external aspects of the tympanic membrane during swallowing. During breathing, however, the eustachian tube is closed. The eustachian tube cartilage bulges into the lateral nasopharyngeal wall at the torus tubarius. A C-shaped prominence is seen radiographically near the torus tubarius ( Fig. 14-4 ). The salpingopharyngeal fold overlying the salpingopharyngeal muscle courses inferiorly from the torus along the lateral pharyngeal wall to the level of the soft palate. The posterior nasopharyngeal wall has a variably nodular surface because of underlying adenoidal tissue.

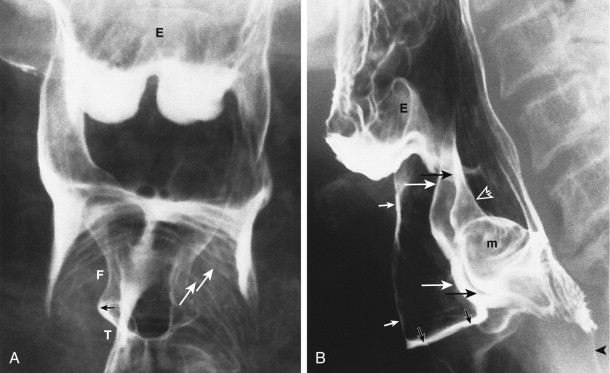
The vertical (pharyngeal) surface of the base of the tongue is variably nodular because of underlying lymphoid tissue of the lingual tonsil (see Fig. 14-1A ). The median glossoepiglottic fold overlies the glossoepiglottic ligament, which courses from the base of the tongue to the epiglottis. The median glossoepiglottic fold divides the space between the tongue and the epiglottis into two sacs, the valleculae ( Fig. 14-5 ; see Fig. 14-1 ). The lateral glossoepiglottic folds form the lateral walls of the valleculae. The pharyngoepiglottic folds course from the posterolateral portion of the valleculae into the lateral pharyngeal wall ( Fig. 14-6 ). These folds overlie the paired stylopharyngeal muscles and form the posterior lateral wall of the valleculae. The valleculae are spaces at rest but disappear during swallowing when the epiglottis inverts and the space behind the base of the tongue communicates freely with the remainder of the oropharynx.

The tonsillar fossa forms part of the lateral oropharyngeal wall. Each tonsillar fossa is bounded anteriorly by a palatoglossal fold (anterior tonsillar pillar; Fig. 14-7 ) and posteriorly by a palatopharyngeal fold (posterior tonsillar pillar) overlying the palatopharyngeal muscle (see Figs. 14-7 and 14-11 ).
The rounded epiglottic tip rises above the level of the valleculae (see Fig. 14-1B and 14-5 ). The aryepiglottic folds connect the epiglottis with the mucosa overlying the muscular processes of the arytenoid cartilages (see Fig. 14-5 ). Occasionally, round bulges are seen in the lower aryepiglottic folds, reflecting the small cuneiform and corniculate cartilages embedded in these folds.
The shape of the hypopharynx is created primarily by its relationship to the posteriorly protruding larynx (see Figs. 14-3 and 14-6B ). Protrusion of the larynx into the pharynx creates two grooves in the anterior lateral hypopharynx—the piriform sinuses (recesses), pear-shaped structures that open posteriorly into the hypopharynx (see Fig. 14-6 ). Each piriform sinus is bounded medially by the aryepiglottic fold and mucosa overlying the muscular process of the arytenoid cartilage and laterally by the hyoid bone, thyrohyoid membrane, and thyroid cartilage.
The lower end of the hypopharynx is collapsed, except during passage of a bolus. The posterior portion of the larynx (including the arytenoid cartilages, arytenoid muscles, and cricoid cartilage) protrudes deeply into the lower hypopharynx (see Fig. 14-3 ). The upper esophageal sphincter (formed predominantly by the cricopharyngeal muscle) is tonically contracted at rest, closing the pharyngoesophageal segment (see Fig. 14-1 ). As a result, the lower hypopharynx is markedly constricted in an anteroposterior direction and is often not appreciated on a frontal radiograph. The arcuate lower border of the hypopharynx seen on the frontal view reflects only the protrusion of the larynx into the hypopharynx (see Fig. 14-3 ).
The squamous mucosa of the lateral and posterior pharyngeal walls is closely apposed to the longitudinally striated inner longitudinal muscle layer and its aponeurosis. Only a thin tunica propria separates the epithelium from the muscle or elastic tissue of the aponeurosis. On double-contrast views, longitudinally oriented lines may therefore be seen in the lateral and posterior pharyngeal walls, reflecting apposition of epithelium to muscle ( Fig. 14-8 ).

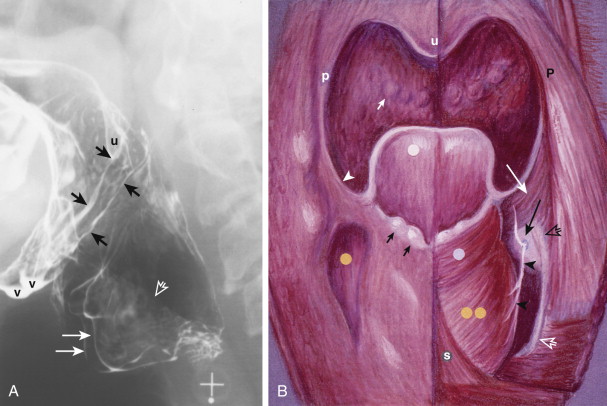
Transversely oriented lines are seen on the anterior hypopharyngeal wall, where redundant squamous mucosa and submucosa overlie the muscular processes of the arytenoid cartilages and cricoid cartilage. Transverse lines and tissue bulging from the anterior wall of the pharyngoesophageal segment had previously been described as a postcricoid venous plexus. However, these radiographic findings are mainly caused by redundant mucosa and submucosa on the anterior hypopharyngeal wall ( Fig. 14-9 ). Demonstration of the redundant postcricoid mucosa on a pharyngogram identifies the location of the cricopharyngeal muscle.

Divisions
The pharynx is arbitrarily divided into three parts—the nasopharynx (epipharynx), oropharynx (mesopharynx), and laryngopharynx (hypopharynx). The nasopharynx is primarily a respiratory tract structure continuous anteriorly with the nasal cavity. The superior and posterior walls of the nasopharynx abut the basisphenoid and basilar part of the occipital bone. The nasopharynx is separated inferiorly from the oropharynx by the soft palate (see Figs. 14-4 and 14-7 ). The velopharyngeal portal is the opening between the nasopharynx and oropharynx.
The oropharynx and hypopharynx are the divisions of the pharynx that participate in swallowing. The oral cavity opens into the oropharynx at the palatoglossal isthmus at the level of the anterior tonsillar pillars (palatoglossal folds; see 14-7A ). The oropharynx lies posterior to the oral cavity, extending craniocaudally from the soft palate to its arbitrary division from the hypopharynx at the level of the hyoid bone. The three divisions of the pharynx are arbitrary because the soft palate and hyoid bone change position with phonation, swallowing, and respiration. Therefore, a better dividing line between the oropharynx and hypopharynx is the pharyngoepiglottic fold (see Fig. 14-6 ), a mucosal fold overlying the stylopharyngeal muscle. The base of the tongue (see Fig. 14-1B ) forms the lower anterior wall of the oropharynx.
The hypopharynx lies behind and lateral to the larynx, extending from the level of the pharyngoepiglottic fold to the lower border of the cricopharyngeal muscle at the level of the inferior margin of the cricoid cartilage. The hypopharynx communicates with the larynx at the laryngeal aditus, formed by the epiglottis, aryepiglottic folds, and mucosa overlying the muscular process of the paired arytenoid cartilages (see Fig. 14-5B ). The hypopharynx communicates with the cervical esophagus at the pharyngoesophageal segment, whose walls are surrounded by the posterior lamina of the cricoid cartilage and cricopharyngeal muscle (see Fig. 14-9 ).
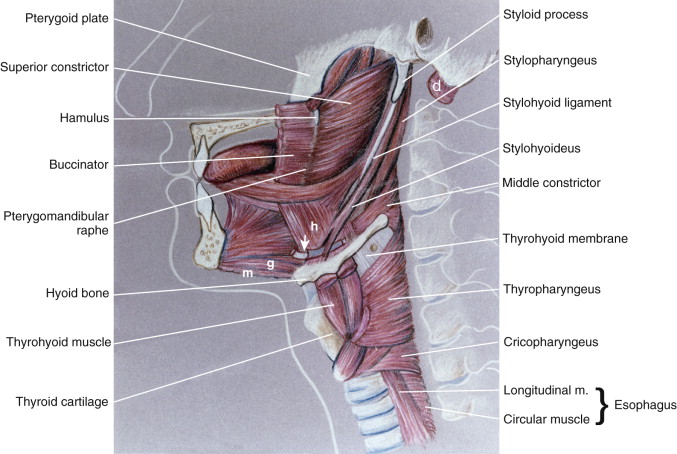
Muscles
Pharyngeal function depends on coordinated, sequential contraction of the extrinsic muscles of the pharynx, which arise from the skull base, neck, tongue, mandible, and hyoid bone, and the intrinsic skeletal muscles of the pharynx and larynx ( Fig. 14-10 ; Table 14-1 ). The pharynx and larynx are suspended as a unit from the skull base, tongue, mandible, and hyoid bone. The suspensory muscles of the hyoid bone (the suprahyoid muscles) include the following (with their cranial nerve innervations in parentheses): from the tongue, mandible, or both, the anterior belly of the digastric muscle (V3), geniohyoid muscle (XII, via C1-2), hyoglossal muscle (XII), and mylohyoid muscle (V3); and from the skull base, the posterior belly of the digastric muscle (VII) and stylohyoid muscle (VII). The major function of the suprahyoid muscle group related to swallowing is to elevate and fix the hyoid bone, a motion that contributes to elevating and widening the pharynx, tilting the epiglottis, and opening the pharyngoesophageal segment during passage of a bolus.
Related posts:
 Abdominal Calcifications
Abdominal Calcifications
 Computed Tomography Enterography
Computed Tomography Enterography
 Malignant Tumors of the Small Bowel
Malignant Tumors of the Small Bowel
 Perfusion Computed Tomography and Magnetic Resonance Imaging in the Abdomen and Pelvis
Perfusion Computed Tomography and Magnetic Resonance Imaging in the Abdomen and Pelvis
 Ulcerative and Granulomatous Colitis: Idiopathic Inflammatory Bowel Disease
Ulcerative and Granulomatous Colitis: Idiopathic Inflammatory Bowel Disease
 Anatomy and Imaging of the Peritoneum and Retroperitoneum
Anatomy and Imaging of the Peritoneum and Retroperitoneum
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


