Oral cavity cancer comprises nearly 30% of all malignant tumors of the head and neck. After a definitive diagnosis has been made, imaging is essential for staging the primary tumor by evaluating submucosal spread and invasion of adjacent structures, and to identify nodal or distant metastasis. Oral cavity anatomy is one of the most complex in the head and neck. Therefore, knowledge of anatomic subsites and spread patterns is critical for accurate staging. This article begins with a discussion of imaging techniques, and then presents a detailed review of normal anatomy followed by imaging’s role in tumor staging highlighting potential pitfalls.
Key points
- •
Staging OC tumors requires knowledge of OC anatomy, the OC subsites, and tumor spread patterns.
- •
Radiologists should always assess for features that would upstage to a T4a disease, including invasion of the extrinsic tongue muscles or mandible, and features that upstage to potentially unresectable T4b disease, including involvement of the masticator space, skull base, and encasement of the internal carotid artery.
- •
This article reviews the detailed imaging anatomy of the OC, and epidemiology, staging, and surveillance for OCSCC.
Introduction and epidemiology
Oral cavity (OC) cancer comprises nearly 30% of all malignant tumors of the head and neck. A total of 90% of cases are squamous cell carcinoma (SCC). The remaining 10% represent minor salivary gland neoplasms, melanoma, lymphoma, and rare varieties of squamous cell and odontogenic tumors. Oral cavity cancer is the sixth leading cause of cancer-related mortality in the world. Although it only accounts for a small percentage (0.6%–5%) of cancers in Western societies, it represents nearly 45% of cancers in certain countries, such as India, secondary to risk factors, such as betel nut chewing. Oral cavity cancer occurs most commonly in middle aged and elderly individuals. However, recent evidence suggests an increased incidence in younger individuals (<40 years) from 3% in 1973 to 6% in 1993. The primary causative risk factors in North America include alcohol and tobacco, which are independent and synergistic. Human papillomavirus is strongly associated with oropharyngeal cancers, but only a minority of OC cancers. Oral cancer is often diagnosed at a late stage contributing to the low 5-year survival rates, hovering at 50 60% overall and as low as 22% for late stage.
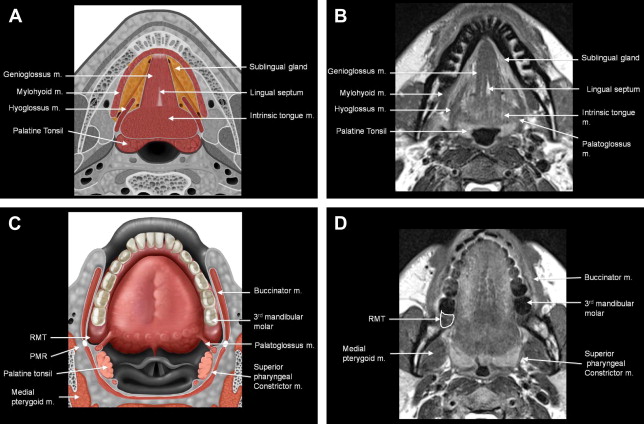
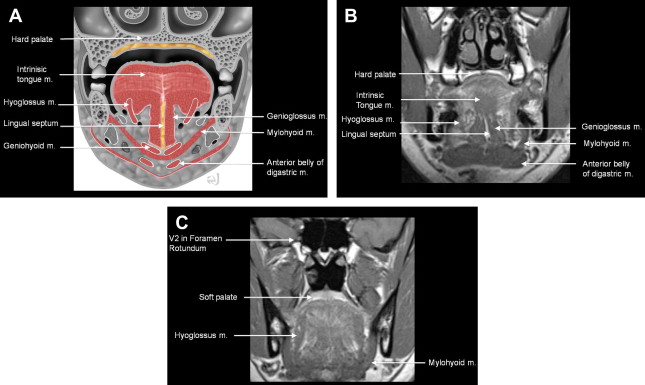
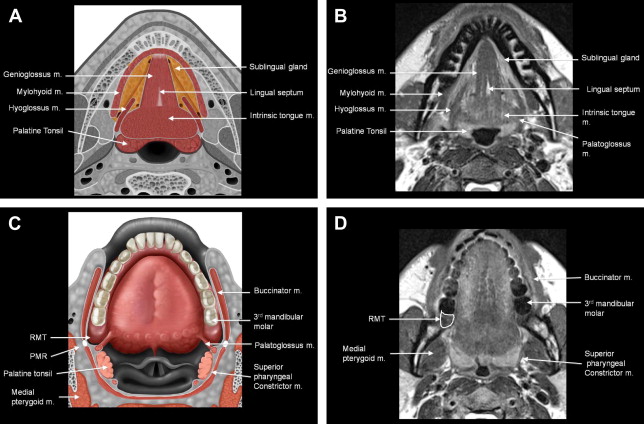
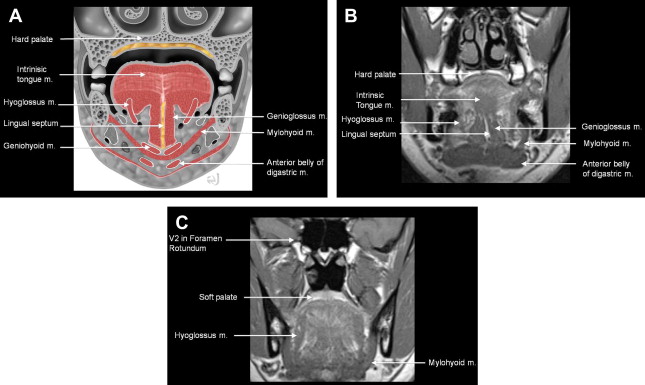
The OC is the most anterior subdivision of the aerodigestive tract with a wide variety of tissue types for such a small region. The posterior OC is separated from the oropharynx (OP) by an imaginary ring drawn across the circumvallate papillae, anterior tonsillar pillars, and junction of the hard and soft palate. This is a critical distinction because carcinomas in the OC versus OP differ in presentation, treatment, and prognosis. However, it is not uncommon for OC tumors to spread to the OP and vice versa. The remaining boundaries of the OC include the lips anteriorly; the cheeks laterally; the hard palate and superior alveolar ridge superiorly; and the inferior alveolar ridge and mylohyoid muscle inferiorly ( Figs. 1 and 2 ). The oral mucosal space refers to the nonkeratinized stratified squamous epithelium lining the entire OC including the buccal (cheek), gingival (gums), palatal, and lingual surfaces. These are the potential sites for SCC. In addition, subepithelial collections of minor salivary glands are found throughout the OC, most commonly along the inner surface of the lip, buccal mucosa, and hard palate. These are potential sites for minor salivary gland neoplasms, such as adenoid cystic and mucoepidermoid carcinomas.
The OC is readily accessible, so oral cancer screening and initial evaluation should be accomplished by clinical examination. Changes in the mucosa are easily identified and evaluated. After a definitive diagnosis has been made, imaging is essential for staging the primary tumor by evaluating submucosal spread and invasion of adjacent structures, and to identify nodal or distant metastasis. OC anatomy is one of the most complex in the head and neck; therefore, knowledge of anatomic subsites and spread patterns is critical for accurate staging. This article begins with a discussion of imaging techniques, and then presents a detailed review of normal anatomy followed by imaging’s role in tumor staging highlighting potential pitfalls ( Table 1 ).
| Pitfall | Advice |
|---|---|
| Upstage to T4a: Misinterpreting odontogenic disease as mandible invasion | Thin section bone CT with multiplanar reformats |
| Upstage to T4a: Misinterpreting atrophic edentulous mandible as tumor invasion/destruction | Thin section bone CT with multiplanar reformats |
| Upstage to T4a: Not recognizing extrinsic tongue muscle involvement significance rather than intrinsic | Know anatomy of hyoglossus and genioglossus MR imaging may help in difficult cases |
| Hard palate primary: Understaging with CT | Recommend MR imaging for all cases being considered for resection to delineate tumor spread |
| PET-CT too early after surgery or biopsy | Wait at least 8 wk |
| Upstaging to T4b: Overcalling involvement of masticator space | Tumor may bulge rather than invade medial pterygoid muscle. Most surgeons will still attempt resection for medial pterygoid involvement |
Introduction and epidemiology
Oral cavity (OC) cancer comprises nearly 30% of all malignant tumors of the head and neck. A total of 90% of cases are squamous cell carcinoma (SCC). The remaining 10% represent minor salivary gland neoplasms, melanoma, lymphoma, and rare varieties of squamous cell and odontogenic tumors. Oral cavity cancer is the sixth leading cause of cancer-related mortality in the world. Although it only accounts for a small percentage (0.6%–5%) of cancers in Western societies, it represents nearly 45% of cancers in certain countries, such as India, secondary to risk factors, such as betel nut chewing. Oral cavity cancer occurs most commonly in middle aged and elderly individuals. However, recent evidence suggests an increased incidence in younger individuals (<40 years) from 3% in 1973 to 6% in 1993. The primary causative risk factors in North America include alcohol and tobacco, which are independent and synergistic. Human papillomavirus is strongly associated with oropharyngeal cancers, but only a minority of OC cancers. Oral cancer is often diagnosed at a late stage contributing to the low 5-year survival rates, hovering at 50 60% overall and as low as 22% for late stage.
The OC is the most anterior subdivision of the aerodigestive tract with a wide variety of tissue types for such a small region. The posterior OC is separated from the oropharynx (OP) by an imaginary ring drawn across the circumvallate papillae, anterior tonsillar pillars, and junction of the hard and soft palate. This is a critical distinction because carcinomas in the OC versus OP differ in presentation, treatment, and prognosis. However, it is not uncommon for OC tumors to spread to the OP and vice versa. The remaining boundaries of the OC include the lips anteriorly; the cheeks laterally; the hard palate and superior alveolar ridge superiorly; and the inferior alveolar ridge and mylohyoid muscle inferiorly ( Figs. 1 and 2 ). The oral mucosal space refers to the nonkeratinized stratified squamous epithelium lining the entire OC including the buccal (cheek), gingival (gums), palatal, and lingual surfaces. These are the potential sites for SCC. In addition, subepithelial collections of minor salivary glands are found throughout the OC, most commonly along the inner surface of the lip, buccal mucosa, and hard palate. These are potential sites for minor salivary gland neoplasms, such as adenoid cystic and mucoepidermoid carcinomas.
The OC is readily accessible, so oral cancer screening and initial evaluation should be accomplished by clinical examination. Changes in the mucosa are easily identified and evaluated. After a definitive diagnosis has been made, imaging is essential for staging the primary tumor by evaluating submucosal spread and invasion of adjacent structures, and to identify nodal or distant metastasis. OC anatomy is one of the most complex in the head and neck; therefore, knowledge of anatomic subsites and spread patterns is critical for accurate staging. This article begins with a discussion of imaging techniques, and then presents a detailed review of normal anatomy followed by imaging’s role in tumor staging highlighting potential pitfalls ( Table 1 ).
| Pitfall | Advice |
|---|---|
| Upstage to T4a: Misinterpreting odontogenic disease as mandible invasion | Thin section bone CT with multiplanar reformats |
| Upstage to T4a: Misinterpreting atrophic edentulous mandible as tumor invasion/destruction | Thin section bone CT with multiplanar reformats |
| Upstage to T4a: Not recognizing extrinsic tongue muscle involvement significance rather than intrinsic | Know anatomy of hyoglossus and genioglossus MR imaging may help in difficult cases |
| Hard palate primary: Understaging with CT | Recommend MR imaging for all cases being considered for resection to delineate tumor spread |
| PET-CT too early after surgery or biopsy | Wait at least 8 wk |
| Upstaging to T4b: Overcalling involvement of masticator space | Tumor may bulge rather than invade medial pterygoid muscle. Most surgeons will still attempt resection for medial pterygoid involvement |
Imaging protocols
The choice of imaging modality is often determined by the clinical question and treatment options. Computed tomography (CT) is generally the workhorse modality for OC cancer. It can be acquired within minutes limiting motion artifact, and can easily be reformatted in coronal and sagittal planes. CT is also preferred to evaluate for early cortical bone involvement. MR imaging may complement CT of the OC because it offers advantages in delineating soft tissue anatomy, especially where accurate tumor extent is critical for surgical planning and negative margins. MR imaging may also be preferable in patients with excessive dental amalgam artifact obscuring the primary tumor and tumor extent. The overall accuracy of CT versus MR imaging for T staging is comparable. However, many subsites, especially the hard palate, can be understaged with CT and therefore MR imaging is invaluable for accurately defining margins and evaluating for perineural extension. CT is more affected by artifact caused by dental metals, whereas MR imaging is more affected by artifact caused by movements of the patient. Most studies that have compared the accuracy of CT and MR imaging for the assessment of the neck have also found no difference. Although positron emission tomography (PET) and PET-CT have the potential to increase sensitivity for nodal disease, some authors have found that the diagnostic accuracy for OC nodal metastasis did not improve significantly compared with CT or MR imaging alone.
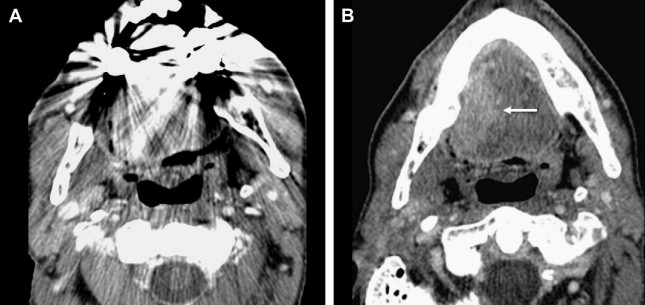
Although protocols vary based on institution, my CT protocol includes 1.25-mm helical images after injection of intravenous contrast, reconstructed at 2.5 mm from the orbits through the thoracic inlet, with routine use of sagittal and coronal reformations. I also obtain a second set of images through the OC with delayed mucosal enhancement and butterfly angled images to decrease dental amalgam artifact ( Fig. 3 ).
An ideal MR imaging protocol includes axial, sagittal, and coronal images obtained with a dedicated neck coil and section thickness of 4 mm or less. Optimal field of view is 16 to 18 cm on T1- and 18 to 20 cm on T2-weighted images allowing for improved signal-to-noise ratio. Three planes of precontrast T1-weighted imaging are desirable to delineate normal anatomy and obliteration of fat and muscle planes. Postgadolinium T1-weighted fat-saturated sequences are especially useful for delineating enhancing tumor margins from intrinsically high signal intensity fat, and in the evaluation for perineural tumor. However, fat suppression can result in artifacts with signal loss and distortion. In this case, I prefer to add postgadolinium sequences without fat saturation.
Staging
The American Joint Committee on Cancer (AJCC) staging for lip and OC can be found in Table 2 . This TNM staging system is only used for epithelial tumors including SCC and minor salivary gland carcinoma. T1, T2, and T3 lesions of the OC are distinguished based on 2-cm increments in size. Patterns of invasion are used to upstage to a T4a or T4b lesion. The primary considerations to upstage to T4a disease include bone invasion (mandible or maxilla) or involvement of the extrinsic tongue muscles. It is critical, therefore, that the radiologist be able to routinely identify the extrinsic tongue muscles. The sixth edition of the AJCC Cancer Staging Manual modified OC staging by the addition of T4b, which denoted unresectable disease. Since that time, the seventh edition of the AJCC has replaced the “resectable” versus “unresectable” terminology for T4a and T4b respectively to “moderately advanced” and “very advanced” disease. T4b still refers to tumor invasion of the masticator space, pterygoid plates, or skull base and tumor encasement of the internal carotid artery. The criteria for nodal staging of OC are identical to the criteria for other sites in the pharynx and larynx, with the exception of nasopharynx.
| Primary Tumor (T) | |
| TX | Primary tumor cannot be assessed |
| T0 | No evidence of primary tumor |
| Tis | Carcinoma in situ |
| T1 | Tumor 2 cm or less in greatest dimension |
| T2 | Tumor more than 2 cm but not more than 4 cm in greatest dimension |
| T3 | Tumor more than 4 cm in greatest dimension |
| T4a | Moderately advanced local disease (lip) Tumor invades through cortical bone, inferior alveolar nerve, floor of mouth, or skin of face, i.e., chin or nose (oral cavity) Tumor invades adjacent structures only (e.g., through cortical bone, [mandible or maxilla] into deep [extrinsic] muscle of tongue [genioglossus, hyoglossus, palatoglossus, and styloglossus], maxillary sinus, skin of face) |
| T4b | T4b Very advanced local disease Tumor invades masticator space, pterygoid plates, or skull base and/or encases internal carotid artery |
| Note: Superficial erosion alone of bone/tooth socket by gingival primary is not sufficient to classify a tumor as T4 | |
| Regional Lymph Nodes (N) | |
| NX | Regional lymph nodes cannot be assessed |
| N0 | No regional lymph node metastasis |
| N1 | Metastasis in a single ipsilateral lymph node, 3 cm or less in greatest dimension |
| N2 | Metastasis in a single ipsilateral lymph node, more than 3 cm but not more than 6 cm in greatest dimension; or in multiple ipsilateral lymph nodes, none more than 6 cm in greatest dimension; or in bilateral or contralateral lymph nodes, none more than 6 cm in greatest dimension |
| N2a | Metastasis in single ipsilateral lymph node more than 3 cm but not more than 6 cm in greatest dimension |
| N2b | Metastasis in multiple ipsilateral lymph nodes, none more than 6 cm in greatest dimension |
| N2c | Metastasis in bilateral or contralateral lymph nodes, none more than 6 cm in greatest dimension |
| N3 | Metastasis in a lymph node more than 6 cm in greatest dimension |
| Distant Metastasis (M) | |
| M0 | No distant metastasis |
| M1 | Distant metastasis |
Additional Prognostic Indicators and Trends in Treatment Important for Staging
Tumor thickness and depth of invasion are important prognostic factors and surgical planning tools in OC cancer that are not included in the T staging of the AJCC. Tumor thickness and depth of invasion have been associated with local recurrence and survival for cancer of the oral tongue. The exact depth of invasion that predicts nodal disease is not clear, but several studies have suggested that tumor thickness greater than 4 mm increases the chance of cervical metastasis. Elective neck dissection for early T1-T2 N0 disease continues to be investigated. Clinically and radiographically occult nodal disease found only at surgery increases the risk of recurrence and decreases 5-year survival from 82% to 53%. Furthermore, Kligerman and colleagues showed that a prophylactic neck dissection in patients with low-volume primary and N0 neck reduced recurrence rate from 33% to 12%, compared with those in whom the neck was treated with watchful waiting. Some authors advocate a prophylactic neck dissection for all OC cancers, regardless of depth of invasion. Others recommend a staging supraomohyoid neck dissection for all patients with T2 disease at the primary site, and T1 disease with greater than 4 mm depth of invasion. Because 70% to 80% of neck dissection specimens are negative for regional metastatic disease, recently some authors advocate a sentinel node biopsy.
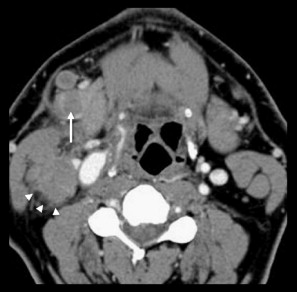
Perineural invasion and lymphocytic response are additional histopathologic parameters that are not accounted for in the current AJCC staging system. Extracapsular spread (ECS) may have a significant impact on the prognosis of patients with regional disease, with up to 50% reduction in survival. On imaging, ill-defined margins of the lymph node and stranding are the biggest clues to ECS ( Fig. 4 ). Patients with ECS are commonly treated with adjuvant radiation and chemotherapy.
Superficial carcinomas of the OC can be treated with excellent cure rates with either radiation or surgery. However, because surgical cure can be achieved rapidly with minimal morbidity, it is often preferred. Advanced disease is often managed with multimodality therapy. Surgery with or without reconstruction coupled with preoperative or postoperative radiation therapy is often used. Most centers perform surgery followed by postoperative radiation because of the higher rate of postoperative complications with preoperative radiation treatment. Although primary surgical management has been advocated for most advanced OC cancer, recent evidence suggests that primary chemoradiotherapy may be effective for selected T4 patients, especially in cases of “functional irresectability,” such as patients requiring total glossectomy.
Related posts:
 Introduction to the Imaging and Staging of Cancer
Pitfalls in the Staging of Cancer of Nasopharyngeal Carcinoma
Introduction to the Imaging and Staging of Cancer
Pitfalls in the Staging of Cancer of Nasopharyngeal Carcinoma
 Pitfalls in the Staging of Cancer of the Oropharyngeal Squamous Cell Carcinoma
Pitfalls in the Staging of Cancer of Thyroid
Pitfalls in the Staging of Cervical Lymph Node Metastasis
Pitfalls in Image Guided Tissue Sampling in the Head and Neck
Pitfalls in the Staging of Cancer of the Oropharyngeal Squamous Cell Carcinoma
Pitfalls in the Staging of Cancer of Thyroid
Pitfalls in the Staging of Cervical Lymph Node Metastasis
Pitfalls in Image Guided Tissue Sampling in the Head and Neck
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


