Post Laryngectomy
Christine M. Glastonbury, MBBS
Key Facts
Terminology
Imaging findings following resection of whole larynx or part of larynx
Most often performed for neoplasm
Total laryngectomy (TL): Larynx completely resected, and neopharynx created
Neopharynx connects oropharynx to esophagus
Trachea no longer communicates with pharynx
Need tracheostomy to breathe, prosthesis to speak
Partial laryngectomy (PL): Conservative surgery
Aim is to preserve voice and breathing
Also to allow swallowing without aspiration
Cordectomy → vertical or horizontal partial laryngectomy → near total laryngectomy
Imaging varies from near-normal to complex reconstruction and deformity
Permanent tracheostomy required only with near total laryngectomy
Top Differential Diagnoses
Larynx trauma
Radiated larynx
Clinical Issues
• Declining use of partial and total laryngectomy with ↑ use of organ preservation chemoradiation
Declining use of open surgery in favor of endoscopic transoral laser surgery (TLS)
Laryngectomy also used for cartilaginous laryngeal tumors, invasive thyroid tumors, salvage after failed chemoradiation, chondronecrosis, nonfunctioning larynx post-treatment
Diagnostic Checklist
Imaging confusion occurs most often with complex appearance of partial laryngectomy
First determine type of procedure
Look for recurrent mass and lymphadenopathy
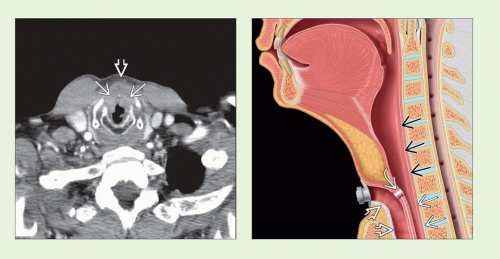 (Left) Axial CECT in patient with T4N0M0 carcinoma of the larynx with subglottic extension  and anterior extension to prelaryngeal tissues and anterior extension to prelaryngeal tissues  . (Right) Sagittal graphic depicts expected appearance after total laryngectomy with all laryngeal cartilages and hyoid resected. Neopharynx . (Right) Sagittal graphic depicts expected appearance after total laryngectomy with all laryngeal cartilages and hyoid resected. Neopharynx  connects oral cavity to esophagus connects oral cavity to esophagus  , while trachea , while trachea  is brought to skin surface as tracheostomy. Tracheoesophageal (TE) voice prosthesis is brought to skin surface as tracheostomy. Tracheoesophageal (TE) voice prosthesis  is a one-way valve that allows speech when patient manually occludes stoma. is a one-way valve that allows speech when patient manually occludes stoma. |
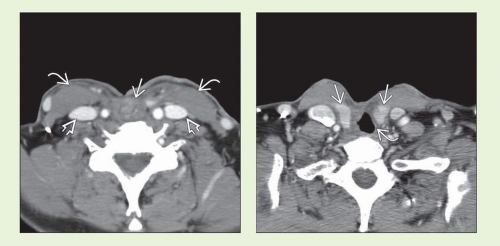 (Left) Axial CECT in same patient following total laryngectomy, right modified neck dissection, & gastric pull-up demonstrates neopharynx as a multilayered midline tubular structure  . Both sternocleidomastoid muscles . Both sternocleidomastoid muscles  and jugular veins and jugular veins  are preserved. (Right) Axial CECT shows new contour of thyroid lobes are preserved. (Right) Axial CECT shows new contour of thyroid lobes  after midline splitting of capsule. If 1 lobe is resected, remaining lobe may be mistaken for node, recurrent mass, or even pseudoaneurysm. Distal anastomosis after midline splitting of capsule. If 1 lobe is resected, remaining lobe may be mistaken for node, recurrent mass, or even pseudoaneurysm. Distal anastomosis  often has slightly irregular contour. often has slightly irregular contour. |
TERMINOLOGY
Definitions
Imaging findings following resection of whole or part of larynx, typically for neoplasm
Total laryngectomy (TL): Larynx resected, neopharynx created, permanent tracheal stoma
Partial laryngectomy (PL): Preserves voice & breathing without permanent tracheostomy
Cordectomy, vertical partial laryngectomy (VPL), horizontal supraglottic laryngectomy (SGL), supracricoid laryngectomy (SCL) with cricohyoidopexy (CHP) or cricohyoidoepiglottopexy (CHEP)
“Pexy” indicates surgical fixation of a structure
Now more often performed as endoscopic transoral laser surgery (TLS) rather than open surgery
IMAGING
General Features
Best diagnostic clue
Abnormal contour of pharyngeal airway (vestibule), absence of soft tissue ± part or whole of one or more cartilages
CT Findings
CECT
Deformed vestibule may be subtle
Soft tissue structures &/or cartilages absent
Arytenoid soft tissue thickening common with PL
Pseudocord scar tissue usually seen with VPL, often with SCL & SGL
Not uncommon to see patchy sclerosis or partial resection of cartilages
Not often helpful or indicative of recurrence
Open resection frequently accompanied by nodal dissection
Imaging Recommendations
Best imaging tool
CECT allows more consistently good quality larynx imaging
MR fraught with motion artifacts
PET: Additive value when recurrence found
Determine systemic disease prior to salvage TL
DIFFERENTIAL DIAGNOSIS
Larynx Trauma
Deformity of cartilages following open or closed injury
Cartilage should not be absent
Radiated Larynx
Mucosal and deep fat space edema
Cartilages present unless chondronecrosis
PATHOLOGY
Staging, Grading, & Classification
Surgeries defined as radical (total laryngectomy) or conservative (cordectomy or partial laryngectomy)
Use of chemoradiation and TLS resulted in marked decline of TL and open PL
Multiple different forms of partial laryngectomy
Defined by plane of resection and form of reconstruction
Cordectomy
Use: Tumor isolated to 1 true vocal cord (TVC) without fixation
Resected: TVC, vocalis muscle, and tendon
Typically performed endoscopically (TLS)
Six different types of TLS cordectomy described
Imaging: Very subtle; may appear normal
Vertical partial laryngectomy
Use: Early stage glottic to anterior commissure (AC) ± arytenoid, without cord fixation
Frontolateral laryngectomy
Use: Tumors to AC without TVC fixation
Resected: Vertical midline segment of thyroid cartilage, TVC (± arytenoid) with ventricle and false cord, AC & small part of contralateral anterior cord
Reconstruction: Contralateral cord mucosa sutured to perichondrium; ipsilateral side may be left to granulate
Imaging: Defect in midline thyroid cartilage, missing AE fold ± ipsilateral arytenoid, dense scar at site of resected cords = pseudocord
Hemilaryngectomy
Use: When more posterior extension of tumor to arytenoid cartilage
Resected: As with frontolateral plus ipsilateral arytenoid, mucosa of AE fold, and thyroid lamina
Reconstruction: Grafts, flap, muscle may be used
Horizontal laryngectomy
Supraglottic laryngectomy
Use: Supraglottic tumor not involving ventricle, normal cord mobility
Resected: Epiglottis, false cords, AE folds, ventricle, upper 1/3 thyroid cartilage, thyrohyoid membrane
Remaining: TVC, arytenoids, lower thyroid cartilage, cricoid
Reconstruction: Thyroid sutured to hyoid (thyrohyoidopexy)
Imaging: Hyoid & thyroid on same plane, redundant mucosa over arytenoids
Extended SGL: SGL plus 1 arytenoid cartilage, tongue base, or pyriform sinus resected
Three-quarters laryngectomy: SGL plus ipsilateral TVC & arytenoid cartilage resected
Remaining: Hyoid, unilateral glottis, cricoid
Supracricoid laryngectomy
Use: More extensive tumor, no cord fixationRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


