15 Preoperative Staging In a dramatic departure from modified radical mastectomy, in the last two decades breast-conserving surgery has become the most frequently selected surgical therapy for breast cancer. Today it accounts for 60% or more of breast cancer operations. Where removal of the breast or large segmental excisions are required, various options are available for reconstruction including silicone or saline prostheses, transverse rectus abdominis myocutaneous flaps, and, for subtotal excisions, latissimus dorsi flaps. Once malignancy has been confirmed, the determination of surgical management relies upon defining the extent of the disease process. Before the era of survey ultrasound and bilateral MRI, the incidence of multifocal and multicentric tumors was still largely unknown. In typical cases the main tumor was detected clinically or through mammographic screening, surgically removed, and histologically evaluated. If clear margins were confirmed, further surgery was withheld and postoperative radiotherapy was instituted. Numerous studies have shown that 20–40% of breast cancer patients have multifocal or multicentric tumors. Most of these lesions are clinically occult. Because premenopausal women are commonly affected, the small multifocal lesions are often undetected by mammography, hidden within the dense fibroglandular tissue. There is evidence from therapeutic studies, however, that the incomplete removal of multifocal carcinomas increases the likelihood of tumor recurrence even when radiotherapy is provided. Consequently, the goal of surgical treatment must be to remove all macroscopic tumor components. Multifocality is not a contraindication to breast-conserving therapy if the foci are in the same quadrant as the index lesion or separated by no more than 4–5 cm, but if no effort is made to locate them, they may remain in the breast, because most breast surgeons keep their excisions as small as possible to achieve good cosmetic results. In recent years the additional information regarding extent of disease has prompted many centers to include MRI (or survey ultrasound) in the preoperative work-up of new or suspected breast cancer patients, because of its high sensitivity in the detection of mammographically occult breast tumors. Because high-resolution ultrasound is also capable of detecting subclinical tumors, tumor extension, and early carcinoma, H. Madjar conducted a prospective study to assess the accuracy of ultra-sound in preoperative staging. The results of the study were very positive, and we have therefore adopted preoperative ultrasound staging as a routine clinical procedure. Tumor size is one of the most important prognostic indicators. In a fatty breast it can be determined with reasonable precision by mammography. In a dense breast, however, superimposed glandular tissue prevents accurate tumor delineation. MRI is also reliable in establishing tumor size, as is a tomographic technique where contrast between background parenchyma and hypoechoic tumor remains. Ultrasound can also define tumor boundaries accurately when a standardized measuring technique is used (Table 15.1). Three orthogonal planes measured from two perpendicular views can be used to compute tumor volume, which may be useful in assessing response to neoadjuvant chemotherapy. The longest axis of a mass should be sought and measured; a measurement perpendicular to this provides the second measurement, and the third measurement can be obtained from the orthogonal view. The measurements should be reported. Also, at the time of excision, particularly if the tumor has been localized before surgery, the radiologist should communicate the orientation of the tumor on the localization images to the surgeon to ensure correlation with the surgical specimen, so that the pathologist can examine representative sections with knowledge of the locations of the various margins. Specimen radiographs and sonograms should be made available to the pathologist for reference in conjunction with preparation of the sections.
Clinical Significance
Tumor Size
Scan plane | Direction of measurement |
Sagittal | Horizontal and vertical |
Transverse | Horizontal |
Radial | Horizontal |
Also: measure in plane of maximum diameter (unless already measured in other standard planes)
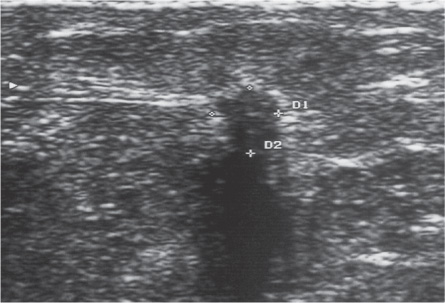
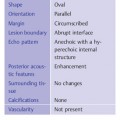
Fig. 15.1 Invasive ductal carcinoma with irregular contours, 5 × 5 mm. Although there is an echogenic rim, the sharp delineation of the tumor from healthy tissues permits a very accurate determination of tumor size.
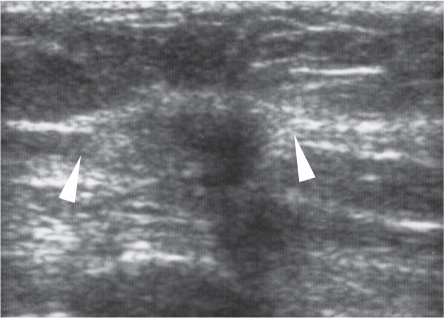
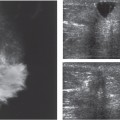
Fig. 15.2 Invasive ductal carcinoma with an irregular shape and ill-defined margins, making it difficult to measure actual tumor size. It can be estimated by including the area of architectural distortion (arrow-heads) around the hypoechoic tumor. Tumor size 15 × 8mm.
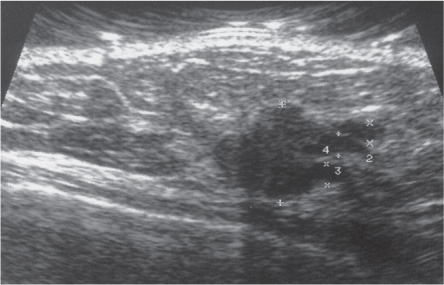
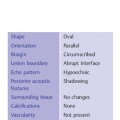
Fig. 15.3 Intraductal component at the periphery of an invasive ductal carcinoma. Radial scan in the upper outer quadrant of the right breast. Intraductal extensions should be included in the measurement of lesion extent.
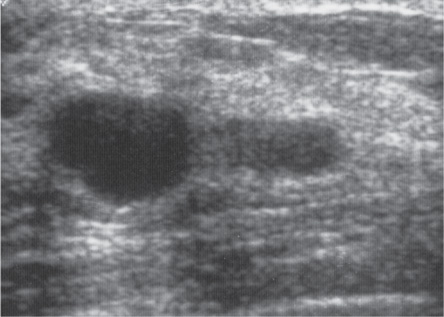
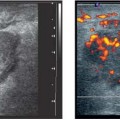
Fig. 15.4 Invasive carcinoma with a lateral, nodular intraductal extension. Radial scan in the lower outer quadrant of the left breast.
The vertical dimension can be difficult to measure in cases where an acoustic shadow obscures the posterior boundary of the tumor. In most cases, dynamic examination with compression, transducer angulation, or increasing the gain setting will help to define the posterior tumor margin. In malignant tumors with irregular contours, the maximum tumor diameter can be easily measured as long as the boundary between the tumor and surrounding tissue is sharply defined (Fig. 15.1). Frequently, however, malignant tumors have ill-defined margins or a hyperechoic rim, in some cases causing a marked discrepancy between the sonographic measurement of the hypoechoic center and the histologically determined tumor size (Fig. 15.2). In those cases, the report might include the dimensions of the hypoechoic portion of the tumor as well as the echogenic part.
Intraductal Carcinomas and Intraductal Components
In the measurement of overall tumor extent, it is important to include any intraductal component that may be present. When the area around an invasive ductal carcinoma is looked at closely, it is common to find microcalcifications or other signs of intraductal extension that directly adjoin the main tumor and permeate the surgical specimen to a variable extent. In these cases it is difficult for the surgeon to decide on an adequate safety margin fortumor excision. When a high-resolution scanner is used for a careful preoperative examination, it is often possible to locate these intraductal extensions at the periphery of the invasive tumor, especially on radial scans, and to ascertain their extent (Figs. 15.3, 15.4).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


