Chapter 8
Rare primary and secondary tumors of the liver
Ersan Altun1, Mohamed El-Azzazi1,2,3,4, and Richard C. Semelka1
1The University of North Carolina at Chapel Hill, Department of Radiology, Chapel Hill, NC, USA
2University of Dammam, Department of Radiology, Dammam, Saudi Arabia
3King Fahd Hospital of the University, Department of Radiology, Khobar, Saudi Arabia
4University of Al Azhar, Department of Radiology, Cairo, Egypt
Lymphoma
- Primary and secondary involvement may occur.
- Primary Liver Lymphoma
- Primary hepatic lymphoma is an extremely rare primary liver tumor.
- Imaging features of primary lymphoma are nonspecific and may mimic imaging features of adenocarcinoma or cholangiocarcinoma. They usually present as solitary masses (Figure 8.1) although multiple foci may sometimes be seen (Figure 8.2)
- They show mildly high signal on T2-WI and moderate to markedly low signal on T1-WI. Central necrosis, which shows increased moderate to markedly high signal on T2-WI, may be seen (Figure 8.1).
- They are hypovascular tumors and usually show progressive heterogeneous enhancement (Figure 8.1). Peripheral thick ring-like soft tissue with or without central necrosis may be present. Early peripheral enhancement with central progressive enhancement on later phases may also be seen. Perilesional enhancement may also be present.
- Secondary Liver Lymphoma
- Secondary involvement of the liver by lymphoma is more common.
- Hodgkin and non-Hodgkin lymphoma involvement may occur in stage IV disease.
- Non-Hodgkin lymphoma is much more common.
- Appearances:
- Large multiple nodules (the most common) (Figure 8.3)
- Solitary nodule
- Diffuse involvement (Figure 8.4)
- On MRI and CT
- Focal Involvement:
- Lesions vary in signal intensity from low to moderately high on T2-WIs.
- Low in signal intensity on T1-WIs.
- Low attenuation on precontrast CT images.
- These lesions are hypovascular. They usually show early peripheral enhancement and later progressive enhancement on postcontrast images. They may also show progressive heterogeneous enhancement on postcontrast images (Figure 8.3)
- Diffuse Involvement:
- Precontrast signal intensity changes are similar to focal involvement.
- Involvement of portal tracts with progressive enhancement is seen (Figure 8.4)
- Differential Diagnosis:
- Cholangiocarcinoma
- Inflammatory myofibroblastic tumor
- Metastases
- Primary Liver Lymphoma
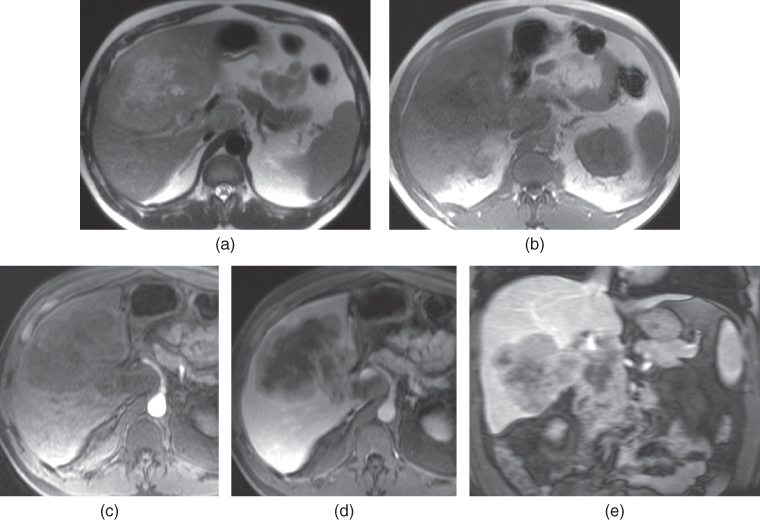
Figure 8.1 Transverse T2-weighted SS-ETSE (a), T1-weighted 2D-GE (b), T1-weighted postgadolinium fat-suppressed hepatic arterial phase (c), hepatic venous phase (d) and interstitial phase (e) 3D-GE images show a large mass with central necrosis in the liver, which represents primary lymphoma. The lesion shows heterogeneous predominantly peripheral enhancement (d) which progresses in the later phases (e). The lesion also extends into the caudate lobe.
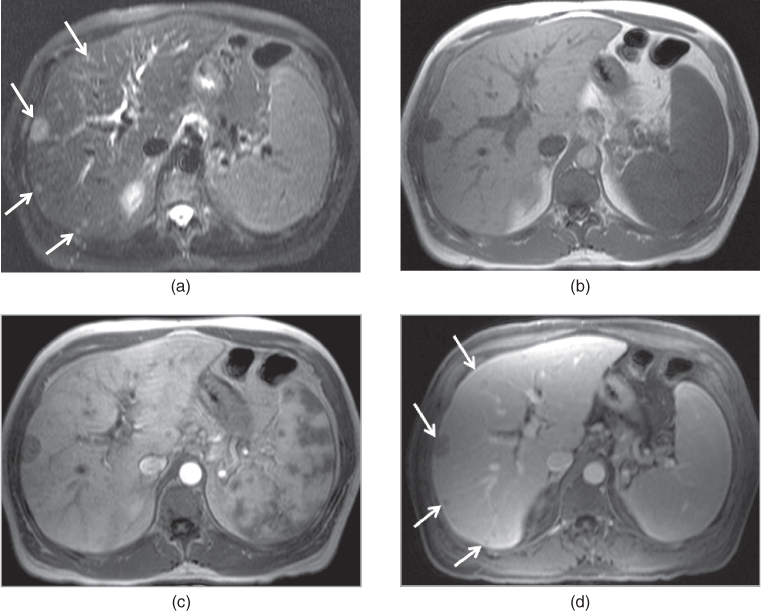
Figure 8.2 Transverse T2-weighted SS-ETSE (a), T1-weighted 2D-GE (b), T1-weighted postgadolinium hepatic arterial dominant phase (c), hepatic venous phase (d) images show multiple foci of primary lymphoma (arrows) in the liver. The lesions show mild enhancement on postgadolinium images.
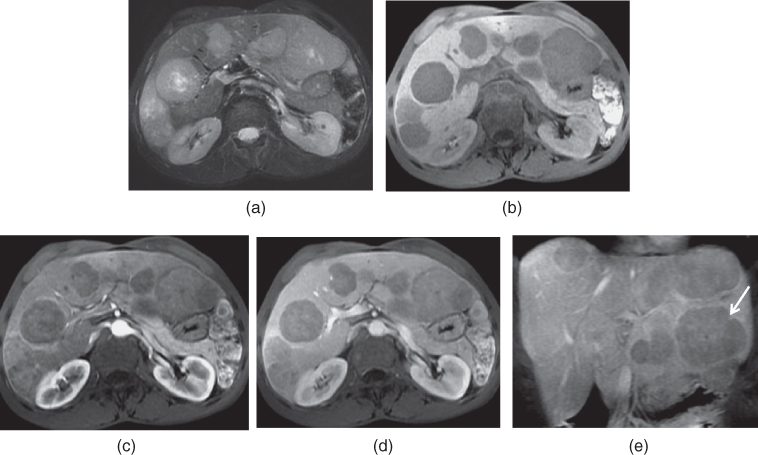
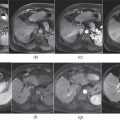
Figure 8.3 Transverse T2-weighted fat-suppressed SS-ETSE (a), T1-weighted fat-suppressed 3D-GE (b), T1-weighted postgadolinium fat-suppressed hepatic arterial dominant phase (c), hepatic venous phase (d) and coronal interstitial phase (e) 3D-GE images show multiple foci of secondary lymphoma in the liver and spleen (arrow, e) due to Non-Hodgkin lymphoma. The lymphoma foci show mild heterogeneous enhancement.
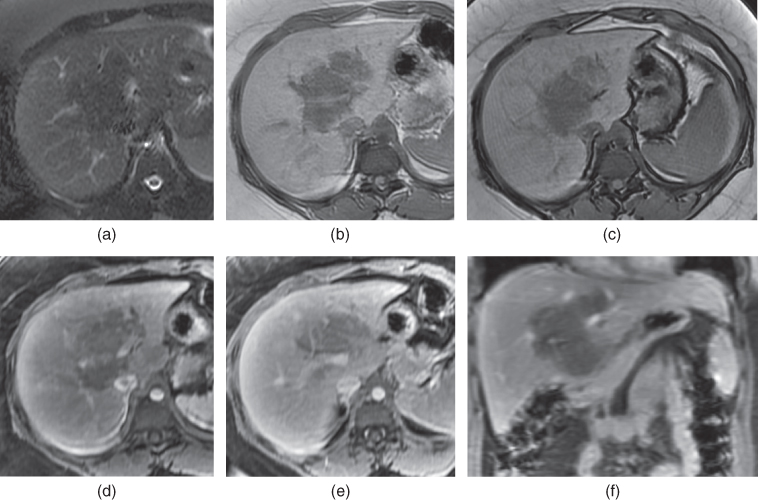
Figure 8.4 Transverse T2-weighted fat-suppressed SS-ETSE (a), T1-weighted in-phase (b) and out-of-phase (c) 2D-GE, T1-weighted postgadolinium fat-suppressed hepatic arterial dominant phase (d), hepatic venous phase (e) and coronal interstitial phase (f) 3D-GE images show an infiltrating lymphoma in the porta hilum extending along the portal tracts. The lymphoma shows low T2 signal due to its high cellular content and shows mild enhancement due to its hypovascularity.
Multiple myeloma
- Focal deposits of multiple myeloma rarely occur in the liver and most often in the setting of disseminated disease.
- The liver is the most commonly involved solid organ in the body.
- Focal involvement presents as nodular lesions in the liver. The lesions may vary in size and large lesions measuring more than 5 cm may also be seen.
- Diffuse involvement presents as involvement of portal tracts without formation of focal nodules.
- On MRI and CT:
- Imaging appearances of lesions are not specific.
- Focal nodular lesions demonstrate mild to moderately hyperintense on T2-WI and variable signal intensities on T1-WIs. High signal intensity on T1-WI may develop secondary to high protein content of lesions. These lesions show low attenuation on CT. These lesions demonstrate progressive enhancement on postcontrast images although they may occasionally be hypervascular (Figure 8.5).
- Diffuse involvement may be seen as hepatomegaly and/or infiltration of portal tracts with progressively enhancing tissue.
- Imaging appearances of lesions are not specific.
- Differential Diagnosis:
- Metastases
- Lymphoma
- Cholangiocarcinoma
- Metastases
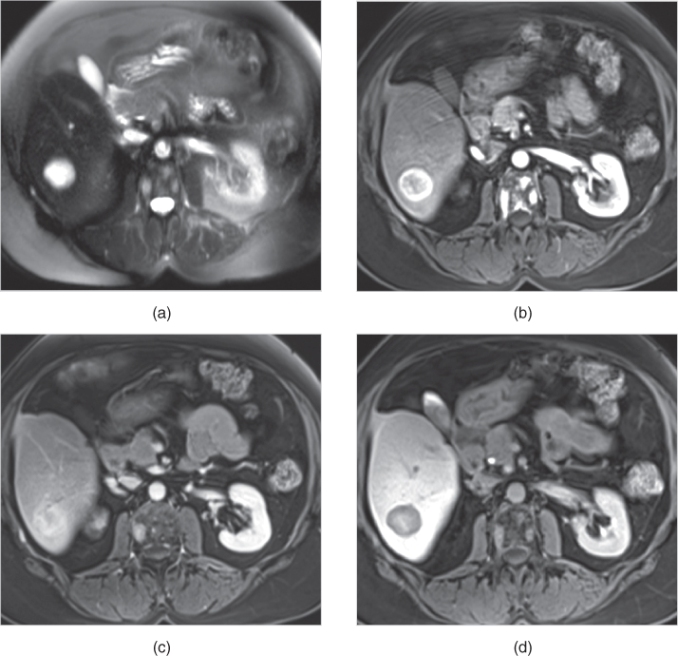
Figure 8.5 Transverse T2-weighted fat-suppressed SS-ETSE (a), T1-weighted postgadolinium hepatic arterial dominant phase (b), hepatic venous phase (c) and hepatocyte phase (d) 3D-GE images show a multiple myeloma metastasis in the right lobe of the liver. The metastasis shows markedly high T2 signal (a) and prominent early enhancement (b) due to its hypervascularity. The lesion appears hypointense on the hepatocyte phase acquired 20 min after the administration of gadoxetic acid, since it does not contain hepatocytes. Note the presence of nodular enhancing lesions in the vertebral body secondary to multiple myeloma.
Extramedullary hematopoiesis
- An unusual condition in which red blood cells are produced outside the bone marrow when the production of red blood cells is not sufficient to meet the demand of the body.
- This condition results from myeloproliferative disorders, hemolytic disease, and bone marrow infiltration, which lead to inadequate hematopoiesis. Focal areas of hematopoiesis may develop in various places in the body including the liver, spleen, lymph nodes, paravertebral areas, and even the kidneys or pleura.
- Hepatomegaly may be seen as a finding in patients with hematopoiesis. Focal solitary or multiple lesions may be seen in the liver with extramedullary hematopoiesis. However, infiltrative lesions along the portal tracts (Figure 8.6) or subcapsular lesions may also be detected.
- On CT:
- Homogeneous low attenuation lesions showing mild or no enhancement on the hepatic arterial dominant phase but shows mild to moderate progressive enhancement in the later phases (Figure 8.6).
- On MRI:
- Homogeneous mild to moderate high signal intensity on T2w images.
- Homogeneous low signal intensity on T2w images may also be seen.
- No or mild enhancement in the hepatic arterial dominant phase with mild to moderate progressive enhancement in the later phases (Figure 8.6).
- Homogeneous mild to moderate high signal intensity on T2w images.
- Differential Diagnosis:
- Lymphoma
- Metastases
- Lymphoma
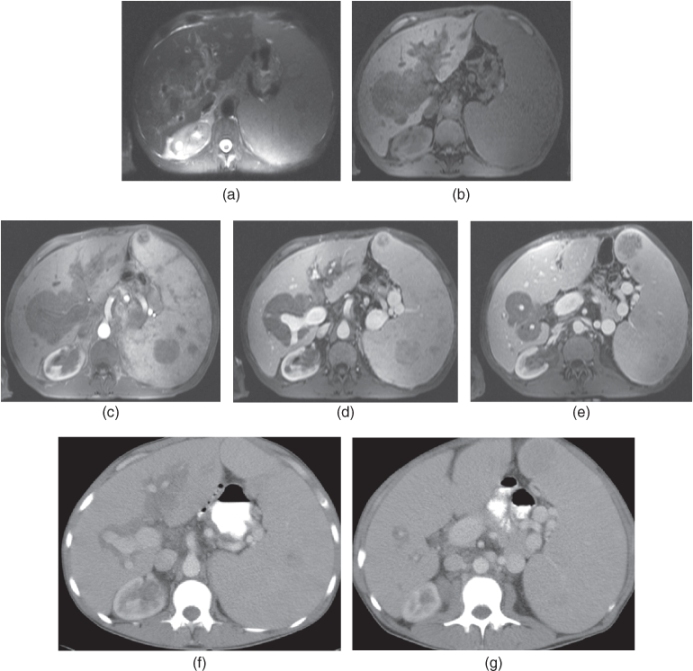
Figure 8.6 Transverse T2-weighted fat-suppressed SS-ETSE (a), T1-weighted fat-suppressed 3D-GE (b), T1-weighted postgadolinium fat-suppressed hepatic arterial dominant phase (c), hepatic venous phase (d) and interstitial phase (e) 3D-GE images show infiltrative midly enhancing mass lesion in the porta hepatis and along the portal tracts. This lesion shows midly high T2 signal. Additionally, multiple foci of moderately enhancing nodular foci are also noted in the enlarged spleen. These lesions develop due to extramedullary hematopoiesis. Postcontrast hepatic venous CT images (f, g) show decrease in the size of periportal infiltration during the treatment. Source: Semelka 2010. Reproduced with permission of Wiley.
Epithelioid hemangioendothelioma (EHE)
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


