Chapter 21 Recognizing Abnormalities of Bone Density
Normal Bone Anatomy
Conventional Radiography
 On conventional radiographs, bones consist of a dense cortex of compact bone, which completely envelopes a less dense medullary cavity containing cancellous bone arranged as trabeculae, separated primarily by blood vessels, hematopoietic cells, and fat. The proportions of cortical versus trabecular bone vary in different skeletal sites and even at different locations in the same bone, i.e., the cortex is naturally thicker in some places than in others.
On conventional radiographs, bones consist of a dense cortex of compact bone, which completely envelopes a less dense medullary cavity containing cancellous bone arranged as trabeculae, separated primarily by blood vessels, hematopoietic cells, and fat. The proportions of cortical versus trabecular bone vary in different skeletal sites and even at different locations in the same bone, i.e., the cortex is naturally thicker in some places than in others.
 The medullary cavity on conventional radiographs appears as a core of less dense, grayish material inside the cortical shell, interlaced with a fine network of bony trabecular markings. The corticomedullary junction is the edge between the inner margin of the cortex and the medullary cavity (Fig. 21-1).
The medullary cavity on conventional radiographs appears as a core of less dense, grayish material inside the cortical shell, interlaced with a fine network of bony trabecular markings. The corticomedullary junction is the edge between the inner margin of the cortex and the medullary cavity (Fig. 21-1).

CT and MRI
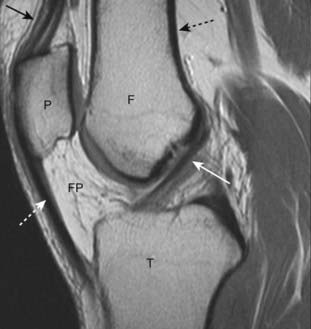
 CT and MRI are able to demonstrate the entire circumference and internal matrix of bone, including, especially with MRI, surrounding soft tissues not visible on conventional radiographs. This is accomplished by computer-aided reformatting and a superior ability to display more subtle differences in tissue densities (Fig. 21-2).
CT and MRI are able to demonstrate the entire circumference and internal matrix of bone, including, especially with MRI, surrounding soft tissues not visible on conventional radiographs. This is accomplished by computer-aided reformatting and a superior ability to display more subtle differences in tissue densities (Fig. 21-2).

The Effect of Bone Physiology on Bone Anatomy
 Bones reflect the general metabolic status of the individual. Their composition requires a protein-containing, collagenous matrix (osteoid) upon which bone mineral, principally calcium phosphate, is transformed into cartilage and bone.
Bones reflect the general metabolic status of the individual. Their composition requires a protein-containing, collagenous matrix (osteoid) upon which bone mineral, principally calcium phosphate, is transformed into cartilage and bone.


 In this chapter, we arbitrarily divide abnormalities of bone density into two major categories based primarily on their appearance on conventional radiographs—those that produce a pattern of either increased or decreased bone density and then subdivide those two patterns by extent of disease: focal versus diffuse (or generalized) changes (Table 21-1).
In this chapter, we arbitrarily divide abnormalities of bone density into two major categories based primarily on their appearance on conventional radiographs—those that produce a pattern of either increased or decreased bone density and then subdivide those two patterns by extent of disease: focal versus diffuse (or generalized) changes (Table 21-1). If MRI were used as the basis for categorization, bone (marrow) disorders could be divided into four other categories:
If MRI were used as the basis for categorization, bone (marrow) disorders could be divided into four other categories:
TABLE 21-1 CHANGES IN BONE DENSITY
| Density | Extent | Examples Used in this Chapter |
|---|---|---|
| Increased Density ↑ | Diffuse | Diffuse osteoblastic metastases |
| Osteopetrosis (rare) | ||
| Focal | Localized osteoblastic metastases | |
| Avascular necrosis of bone | ||
| Paget disease | ||
| Decreased Density ↓ | Diffuse | Osteoporosis |
| Hyperparathyroidism | ||
| Rickets and osteomalacia | ||
| Focal | Localized osteolytic metastases | |
| Multiple myeloma | ||
| Osteomyelitis |
Recognizing a Generalized Increase in Bone Density
 On conventional radiographs and CT, there will be an overall whiteness (sclerosis) to all or most of the bones.
On conventional radiographs and CT, there will be an overall whiteness (sclerosis) to all or most of the bones.
 There is also a loss of visualization of the normal corticomedullary junction because of the abnormally increased density of the medullary cavity relative to the cortex (Fig. 21-3).
There is also a loss of visualization of the normal corticomedullary junction because of the abnormally increased density of the medullary cavity relative to the cortex (Fig. 21-3).

Figure 21-3 Diffuse metastatic disease from carcinoma of the prostate.
The bones are diffusely sclerotic. You can no longer see the normal trabeculae or the junction between the medullary cavity and the cortex as the medullary cavities have been filled in with osteoblastic metastatic disease that obscures these normal boundaries and increases the overall bone density. Contrast this picture with that of Paget disease of the pelvis (see Fig. 21-12).
Carcinoma of the Prostate
 Diffuse, blood-borne, metastatic disease from carcinoma of the prostate is the prototype for generalized increase in bone density. Osteoblastic activity occurs beyond the control of normal physiologic constraints.
Diffuse, blood-borne, metastatic disease from carcinoma of the prostate is the prototype for generalized increase in bone density. Osteoblastic activity occurs beyond the control of normal physiologic constraints.
 With diffuse bone metastases, a so-called superscan may be seen on radionuclide bone scan. The superscan demonstrates high radiotracer uptake throughout the skeleton, with poor or absent renal excretion of the radiotracer (Fig. 21-4).
With diffuse bone metastases, a so-called superscan may be seen on radionuclide bone scan. The superscan demonstrates high radiotracer uptake throughout the skeleton, with poor or absent renal excretion of the radiotracer (Fig. 21-4).




Recognizing a Focal Increase in Bone Density
 Focal sclerotic lesions can affect the cortex and medullary cavity. Those that affect the cortex will usually produce periosteal new-bone formation (periosteal reaction), which leads to an appearance of thickening of the cortex. Those that affect the medullary cavity will result in punctate, amorphous sclerotic lesions surrounded by the normal medullary cavity (Fig. 21-6).
Focal sclerotic lesions can affect the cortex and medullary cavity. Those that affect the cortex will usually produce periosteal new-bone formation (periosteal reaction), which leads to an appearance of thickening of the cortex. Those that affect the medullary cavity will result in punctate, amorphous sclerotic lesions surrounded by the normal medullary cavity (Fig. 21-6).


Carcinoma of the Prostate
 A substance secreted by tumor cells from metastatic carcinoma of the prostate may stimulate osteoblastic activity and produce focal areas of localized increased density, i.e., sclerotic bone lesions. The lesions may also be diffuse. These lesions are most often seen in the vertebrae, ribs, pelvis, humeri, and femora (Fig. 21-7).
A substance secreted by tumor cells from metastatic carcinoma of the prostate may stimulate osteoblastic activity and produce focal areas of localized increased density, i.e., sclerotic bone lesions. The lesions may also be diffuse. These lesions are most often seen in the vertebrae, ribs, pelvis, humeri, and femora (Fig. 21-7). The radionuclide bone scan is currently the study of choice for detecting skeletal metastases, regardless of the suspected primary (Box 21-3).
The radionuclide bone scan is currently the study of choice for detecting skeletal metastases, regardless of the suspected primary (Box 21-3).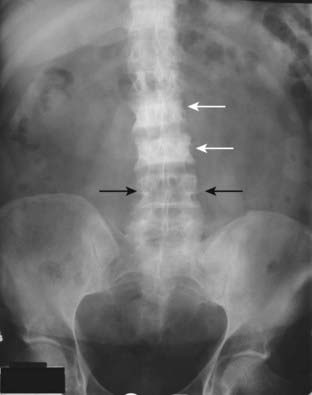
Box 21-3 Finding Metastases to Bone—Bone Scan
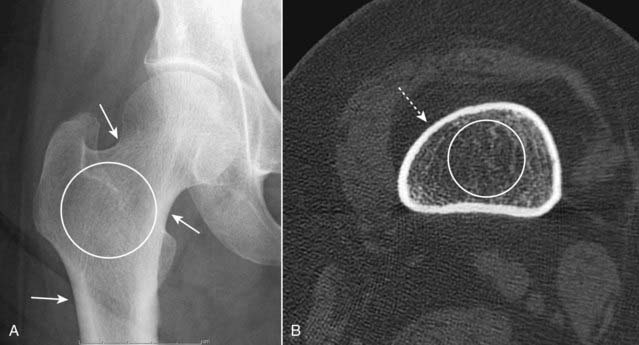
Avascular Necrosis of Bone
 Avascular necrosis (AVN) of bone (also called ischemic necrosis, aseptic necrosis, osteonecrosis) results from cellular death and leads to collapse of the affected bone. It usually involves those bones that have a relatively poor collateral blood supply (e.g., scaphoid in the wrist or the head of the femur) and tends to affect the hematopoietic elements of marrow earliest so that MRI is the most sensitive modality for detecting AVN.
Avascular necrosis (AVN) of bone (also called ischemic necrosis, aseptic necrosis, osteonecrosis) results from cellular death and leads to collapse of the affected bone. It usually involves those bones that have a relatively poor collateral blood supply (e.g., scaphoid in the wrist or the head of the femur) and tends to affect the hematopoietic elements of marrow earliest so that MRI is the most sensitive modality for detecting AVN. There are a myriad of causes of avascular necrosis. Some of the more common are shown in Table 21-2.
There are a myriad of causes of avascular necrosis. Some of the more common are shown in Table 21-2. On conventional radiographs, the region of avascular necrosis appears denser than the surrounding bone. On MRI, there is usually a decrease from the normal high signal produced by fatty marrow (Fig. 21-8).
On conventional radiographs, the region of avascular necrosis appears denser than the surrounding bone. On MRI, there is usually a decrease from the normal high signal produced by fatty marrow (Fig. 21-8).



