Chapter 22 Recognizing Fractures and Dislocations
Recognizing an Acute Fracture
 Everyone, it seems, is fascinated by a broken bone or two. Fractures are a favorite among those learning radiology, perhaps because of how common they are. Fractures due to moderate trauma are much more common than those due to severe trauma or pathologic fractures.
Everyone, it seems, is fascinated by a broken bone or two. Fractures are a favorite among those learning radiology, perhaps because of how common they are. Fractures due to moderate trauma are much more common than those due to severe trauma or pathologic fractures. A fracture is described as a disruption in the continuity of all or part of the cortex of a bone.
A fracture is described as a disruption in the continuity of all or part of the cortex of a bone.• If only a part of the cortex is fractured, it is called incomplete. Incomplete fractures tend to occur in bones that are “softer” than normal such as those in children, or in adults with bone-softening diseases such as osteomalacia or Paget disease (see Chapter 21, Recognizing Abnormalities of Bone Density).
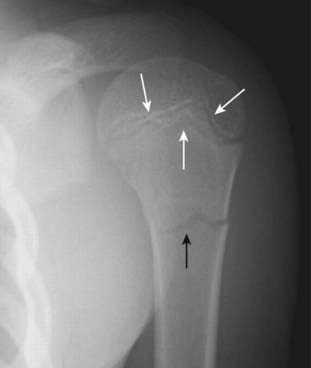
• Examples of incomplete fractures in children are the greenstick fracture, which involves only one part of, but not the entire, cortex, and the torus fracture (buckle fracture), which represents compression of the cortex (Fig. 22-1).

 Radiologic features of acute fractures (
Radiologic features of acute fractures (• Fracture lines, when viewed in the correct plane, tend to be “blacker” (more lucent) than other lines normally found in bones, such as nutrient canals (Fig. 22-2A).
• There may be an abrupt discontinuity of the cortex, sometimes associated with acute angulation of the normally smooth contour of bone (Fig. 22-2B).
• Fracture lines tend to be straighter in their course yet more acute in their angulation than any naturally occurring lines (such as epiphyseal plates) (Fig. 22-3).
• The edges of a fracture tend to be jagged and rough.

 Pitfalls: sesamoids, accessory ossicles, and unhealed fractures (Table 22-1)
Pitfalls: sesamoids, accessory ossicles, and unhealed fractures (Table 22-1)
• Sesamoids are bones that form in a tendon as it passes over a joint. The patella is the largest and most famous sesamoid bone.
• Accessory ossicles are accessory epiphyseal or apophyseal ossification centers that do not fuse with the parent bone.
• Unlike fractures, these small bones are corticated (i.e., there is a white line that completely surrounds the bony fragment) and their edges are usually smooth.
• In the case of sesamoids and accessory ossicles, they are usually bilaterally symmetrical so that a view of the opposite extremity will usually demonstrate the same bone in the same location. They also occur at anatomically predictable sites.
• There are almost always sesamoids present in the thumb, the posterolateral aspect of the knee (fabella), and the great toe (Fig. 22-4B).
TABLE 22-1 DIFFERENTIATING FRACTURES, OSSICLES, AND SESAMOIDS
| Finding | Acute Fracture | Sesamoids and Accessory Ossicles* |
|---|---|---|
| Abrupt disruption of cortex | Yes | No |
| Bilaterally symmetrical | Almost never | Almost always |
| “Fracture line” | Unsharp, jagged | Smooth |
| Bony fragment has a cortex completely around it | No | Yes |
* Old, unhealed fractures will not be bilaterally symmetrical.

Recognizing Dislocations and Subluxations
 In a dislocation, the bones that originally formed the two components of a joint are no longer in apposition to each other. Dislocations occur only at joints (Fig. 22-5A).
In a dislocation, the bones that originally formed the two components of a joint are no longer in apposition to each other. Dislocations occur only at joints (Fig. 22-5A). In a subluxation, the bones that originally formed the two components of a joint are in partial contact with each other. Subluxations also occur only at joints (Fig. 22-5B).
In a subluxation, the bones that originally formed the two components of a joint are in partial contact with each other. Subluxations also occur only at joints (Fig. 22-5B).

TABLE 22-2 DISLOCATIONS OF THE SHOULDER AND HIP
| Shoulder | Hip |
|---|---|
| Anterior, subcoracoid most common | Posterior and superior more common |
| Caused by a combination of abduction, external rotation, and extension | Frequently caused by knee striking dashboard transmitting force to hip |
| Associated with fractures of humeral head (Hill-Sachs lesion) and glenoid (Bankart lesion) | Associated with fractures of posterior rim of the acetabulum |
Describing Fractures
 There is a common lexicon used in describing fractures to facilitate a reproducible description and to assure reliable and accurate communication.
There is a common lexicon used in describing fractures to facilitate a reproducible description and to assure reliable and accurate communication.
TABLE 22-3 HOW FRACTURES ARE DESCRIBED
| Parameter | Terms Used |
|---|---|
| Number of fracture fragments | Simple or comminuted |
| Direction of fracture line | Transverse, oblique (diagonal), spiral |
| Relationship of one fragment to another | Displacement, angulation, shortening, and rotation |
| Open to the atmosphere (outside) | Closed or open (compound) |
How Fractures are Described: by the Number of Fracture Fragments

 If the fracture produces more than two fragments, it is called a comminuted fracture. Some comminuted fractures have special names.
If the fracture produces more than two fragments, it is called a comminuted fracture. Some comminuted fractures have special names.• A segmental fracture is a comminuted fracture in which a portion of the shaft exists as an isolated fragment (Fig. 22-6A).

How Fractures are Described: by the Direction of the Fracture Line (Table 22-4)
 In a transverse fracture, the fracture line is perpendicular to the long axis of the bone. Transverse fractures are caused by a force directed perpendicular to shaft (Fig. 22-7A).
In a transverse fracture, the fracture line is perpendicular to the long axis of the bone. Transverse fractures are caused by a force directed perpendicular to shaft (Fig. 22-7A). In a diagonal or oblique fracture, the fracture line is diagonal in orientation relative to the long axis of the bone. Diagonal or oblique fractures are caused by a force usually applied along the same direction as the long axis of the affected bone (Fig. 22-7B).
In a diagonal or oblique fracture, the fracture line is diagonal in orientation relative to the long axis of the bone. Diagonal or oblique fractures are caused by a force usually applied along the same direction as the long axis of the affected bone (Fig. 22-7B). With a spiral fracture, a twisting force or torque produces a fracture like those that might be caused by planting the foot in a hole while running. Spiral fractures are usually unstable and often associated with soft tissue injuries such as tears in ligaments or tendons (Fig. 22-7C).
With a spiral fracture, a twisting force or torque produces a fracture like those that might be caused by planting the foot in a hole while running. Spiral fractures are usually unstable and often associated with soft tissue injuries such as tears in ligaments or tendons (Fig. 22-7C).TABLE 22-4 DIRECTION OF FRACTURE LINE AND MECHANISM OF INJURY
| Direction of Fracture Line | Mechanism |
|---|---|
| Transverse | Force applied perpendicular to long axis of bone; fracture occurs at point of impact |
| Diagonal (also known as oblique) | Force applied along the long axis of bone; fracture occurs somewhere along shaft |
| Spiral | Twisting or torque injury |

How Fractures are Described: by the Relationship of One Fracture Fragment to Another
 By convention, abnormalities of the position of bone fragments secondary to fractures describe the relationship of the distal fracture fragment relative to the proximal fragment. These descriptions are based on the position the distal fragment would have normally assumed had the bone not been fractured.
By convention, abnormalities of the position of bone fragments secondary to fractures describe the relationship of the distal fracture fragment relative to the proximal fragment. These descriptions are based on the position the distal fragment would have normally assumed had the bone not been fractured. There are four major parameters most commonly used to describe the relationship of fracture fragments. Most fractures display more than one of these abnormalities of position. The four parameters are:
There are four major parameters most commonly used to describe the relationship of fracture fragments. Most fractures display more than one of these abnormalities of position. The four parameters are: Displacement describes the amount by which the distal fragment is offset, front to back and side to side, from the proximal fragment. Displacement is most often described either in terms of percent (the distal fragment is displaced by 50% of the width of the shaft) or by fractions (the distal fragment is displaced half the width of the shaft of the proximal fragment) (Fig. 22-8A).
Displacement describes the amount by which the distal fragment is offset, front to back and side to side, from the proximal fragment. Displacement is most often described either in terms of percent (the distal fragment is displaced by 50% of the width of the shaft) or by fractions (the distal fragment is displaced half the width of the shaft of the proximal fragment) (Fig. 22-8A). Angulation describes the angle between the distal and proximal fragments as a function of the degree to which the distal fragment is deviated from the position it would have assumed were it in its normal position. Angulation is described in degrees and by position (the distal fragment is angulated 15° anteriorly relative to the proximal fragment) (Fig. 22-8B).
Angulation describes the angle between the distal and proximal fragments as a function of the degree to which the distal fragment is deviated from the position it would have assumed were it in its normal position. Angulation is described in degrees and by position (the distal fragment is angulated 15° anteriorly relative to the proximal fragment) (Fig. 22-8B). Shortening describes how much, if any, overlap there is of the ends of the fracture fragments, which translates into how much shorter the fractured bone is than it would be had it not been fractured (Fig. 22-8C).
Shortening describes how much, if any, overlap there is of the ends of the fracture fragments, which translates into how much shorter the fractured bone is than it would be had it not been fractured (Fig. 22-8C).• The term opposite from shortening is distraction, which refers to the distance the bone fragments are separated from each other (Fig. 22-8D).
 Rotation is an unusual abnormality in fracture positioning almost always involving the long bones, such as the femur or humerus. Rotation describes the orientation of the joint at one end of the fractured bone relative to the orientation of the joint at the other end of the same bone.
Rotation is an unusual abnormality in fracture positioning almost always involving the long bones, such as the femur or humerus. Rotation describes the orientation of the joint at one end of the fractured bone relative to the orientation of the joint at the other end of the same bone.• Normally, for example, when the hip joint is pointing forward, the knee joint is also pointing forward.
• If there is rotation about a fracture of the femoral shaft, the hip joint could be pointing forward while the knee joint is oriented in another direction (Fig. 22-9).


How Fractures are Described: by the Relationship of the Fracture to the Atmosphere
 A closed fracture is the more common type of fracture in which there is no communication between the fracture fragments and the outside atmosphere.
A closed fracture is the more common type of fracture in which there is no communication between the fracture fragments and the outside atmosphere.



