Fig. 20.1
Flush aortogram via 4Fr pigtail catheter. A significant stenosis of the right renal artery is confirmed (arrow)
(b)
Place 7-Fr renal double curved introducer guide catheter leaving the tip adjacent to the renal artery ostium (Fig. 20.2).

Fig. 20.2
A 7Fr double curved guide catheter is placed at the ostium of the right renal artery
(c)
Administer 3,000–5,000 units of heparin.
(d)
Cross the stenosis with a 0.014 or 0.018 guide wire alternatively if a protection device is going to be used the lesion is crossed with the filter at this stage (Fig. 20.3).
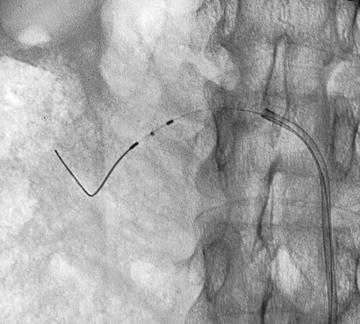
Fig. 20.3
Renal protection device is advanced past the lesion (a 0.018 or 0.014 guide wire alone is an acceptable alternative)
(e)
Pre-dilate the lesion with a 3 mm small platform balloon.
(f)
Introduce the balloon mounted stent (usually 6 × 18 mm). Position checked by gentle contrast injection via the guide catheter.
(g)
Deploy stent allowing for 2–3 mm to project into the aorta (Fig. 20.4).
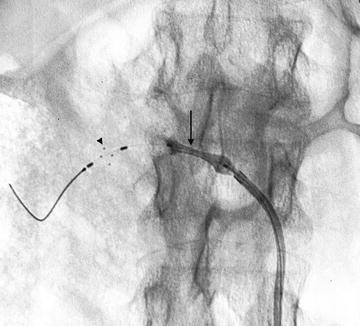
Fig. 20.4
After pre-dilation the balloon mounted stent is deployed (arrow) note the open configuration of the renal protection device (arrowhead)
(h)
Check position with gentle contrast injection via the guide catheter (Fig. 20.5).

Fig. 20.5
Check angiogram via the guide catheter. Guide wire or protection device must remain in the distal vessel so as to allow access to distal vessel if dissection or rupture occurs
(i)
Remove guide wire. Close and remove protection filter if used.
(j)
Manual compression to groin or closure device.
B.Non Ostial Atheromatous Lesions
These rare lesions may respond well to simple angioplasty and stents should be reserved for primary failures (e.g. recoil). Pre-dilation is not required and normally a 6 mm balloon is used.
C.Fibromuscular Dysplasia
Work up should include selective renal angiography as disease affecting the second or third order vessels may be missed by non-invasive methods. Technique is the same as above except that branch lesions may require more complex techniques using “kissing” balloons. Anti-platelets agents are not required.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


