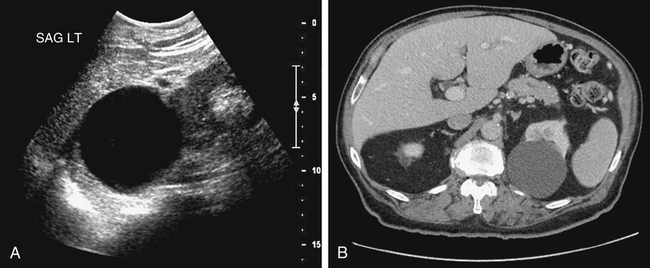
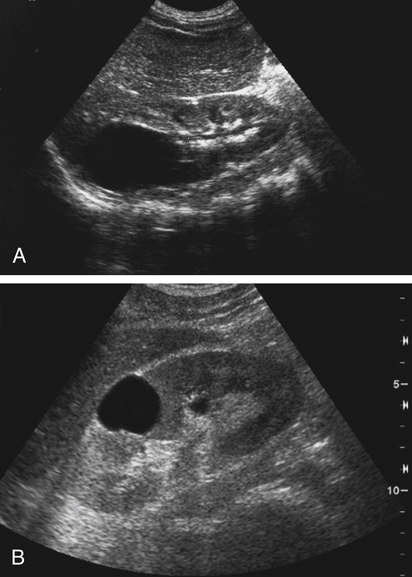
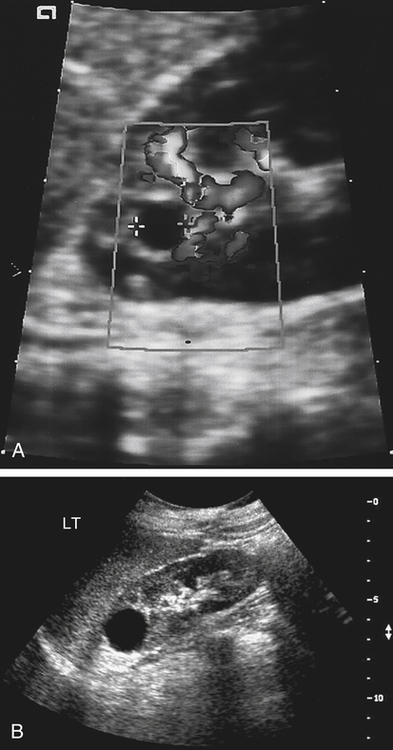
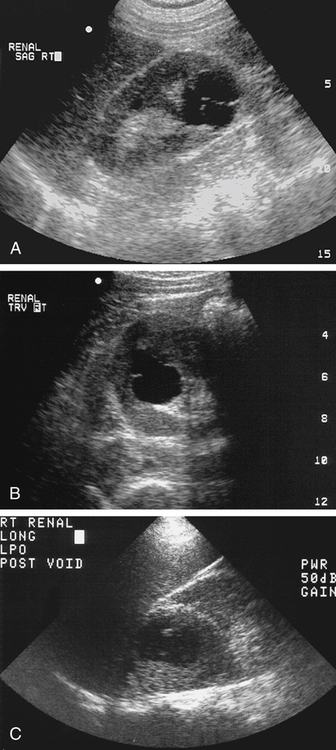
Nancy Chouinard and Ken Marken • Describe and differentiate cystic renal lesions that can be identified sonographically. • Differentiate the sonographic findings of various cystic renal lesions. • Describe the Bosniak renal cyst classifications. • Describe hereditary diseases associated with renal cysts. • List anomalies associated with cystic renal diseases. • Identify Doppler findings associated with cystic lesions. • List symptoms associated with specific renal cystic lesions. CLINICAL SCENARIO A 55-year-old man presented to the emergency department with left upper quadrant pain and hypertension. The initial sonogram demonstrated a left upper quadrant cystic mass of uncertain origin (Fig. 7-1, A). A computed tomography (CT) scan was ordered to establish the organ of origin (Fig. 7-1, B). The sonographer must take particular care to demonstrate accurately whether the cyst is simple or contains features such as thick walls, septations, or nodules. The Bosniak Renal Cyst Classification System is a rubric for determining patient management based on these features.1 Although the system also includes contrast enhancement on CT, the remaining criteria can be helpful in determining appropriate follow-up of a renal cyst demonstrated on a sonogram (Table 7-1). TABLE 7-1 Bosniak Renal Cyst Classification System This chapter explores numerous cystic lesions and cystic diseases of the kidneys. Descriptions of renal neoplasms and the normal sonographic appearance of the kidneys are provided in Chapter 5. The sonographic appearance of a renal cyst should meet the criteria of a simple cyst. The cyst should be anechoic, thin-walled, and round or oval, and the sonogram should show acoustic enhancement posterior to the cyst (Fig. 7-2). Edge shadowing is frequently shown along the lateral margins of the cyst. Doppler analysis of the cyst shows the absence of flow (Fig. 7-3, A). In addition, aside from recognition of a simple cyst, sonography can examine for renal contour or relational anatomy changes. The claw sign is a concavity in the renal contour where the parenchyma appears to be cupping the cyst or mass, indicating that the cyst or mass has a renal origin.2 A renal cyst or mass can cause distortion of the perirenal fat outline or displace adjacent structures (Fig. 7-3, B). Sonographically, a parapelvic cyst appears as a cystic structure arising from the renal sinus. If multiple cysts exist, they may be confused with hydronephrosis. Sonographic differentiation may be made by demonstrating the lack of communication with the cyst or cysts and the collecting system (Fig. 7-4). When a cyst does not meet the criteria of a simple cyst, it may be classified as a complex cyst. Complex cysts may exist within the cortex, medulla, or pelvis. A complex cyst may have one or all of the following findings: a perceptible wall, internal echoes, and variable enhancement. A perceptible wall may include wall (mural) calcification, irregularity, nodularity, or thickening. Internal echoes may include thick viscous fluid, debris, or septations. Septations may result from material aggregating within the fluid or possibly from the inner lining of a cyst separating from its wall (see Table 7-1). These cysts can be hemorrhagic cysts, infected cysts, multilocular or septated cysts, cystic malignancies, or calcified cysts (Fig. 7-5). The diagnosis may be made based on the patient’s symptoms or may require additional imaging with CT or needle aspiration and histologic examination.
Renal Mass
Cystic versus Solid
Classification
Description
1
Simple cysts, 100% benign; no follow-up warranted
2
<3 cm cyst with thin septa or small calcifications; no follow-up warranted
2F
Minimally complicated cyst with suspicious features; follow-up scan recommended, most likely benign
3
Moderately complicated, possible wall nodularity or multiseptated cyst, 50% malignant; surgery recommended because malignancy cannot be ruled out
4
Clearly malignant lesion; surgery recommended
Simple Renal Cysts
Cortical Renal Cysts
Sonographic Findings
Parapelvic Cyst
Sonographic Findings
Complex Renal Cysts
Renal Mass: Cystic versus Solid