Rheumatoid Arthritis
Radiographic Scoring
The modification of radiographic progression is the main criterion for evaluating the efficacy of disease-modifying drugs in rheumatoid arthritis. Since the mid-20th century, various scoring methods have been developed for quantifying the changes depicted by radiographs. The main goal of radiographic scoring in rheumatoid arthritis is the quantification of joint destruction, a largely irreversible process that is the primary measure of disease progression. So far, attempts to measure joint destruction with computer techniques have met with little success. Semiquantitative scoring methods are based largely on erosive changes, and some methods score the percentage of articular surface destruction or the reduction of joint-space width as an indicator of cartilage destruction.
The reliability of radiographic scores depends critically on the quality (readability) of the image. A technically sound radiograph should meet the following criteria:
Use of a high-resolution screen-film combination
Optimum positioning (true dorsoplantar or dorsopalmar projection):
Hands placed flat on the cassette
Patient sitting with the forefeet placed on a cassette lying on the floor
18 × 24-cm format for each hand or for both forefeet
Beam centered on the third metacarpophalangeal joints or between the metatarsophalangeal joints of the big toes
Alternative method: both hands are placed on a 24 × 30-cm cassette and exposed separately
Collimate to include the whole hand and the distal ends of the radius and ulna
Constant exposure parameters
Semioblique views are not strictly necessary
The best approach to radiographic scoring is to include all radiographs of one patient in the evaluation, doing so either in chronological or random order. The latter method is preferred as it reduces misinterpretations based on the assumption of constant progression.
Several different methods of radiographic scoring are presented in the literature:
Global scoring of the patient as a whole
Global scoring of each joint
Separate scoring of erosions and joint-space narrowing
Whereas the first method (e.g., the Kellgren score) is no longer used because it provides only a global assessment, the Larsen scoring system (global score for each joint) or the Sharp system (separate scoring of erosions and joint-space narrowing) are most used in everyday practice and especially within the framework of studies. The Ratingen score is commonly used in everyday practice (outside studies) owing to its relative simplicity. It grades only destructive changes, yielding a separate score for each joint but it does not score joint-space narrowing.
Larsen Score
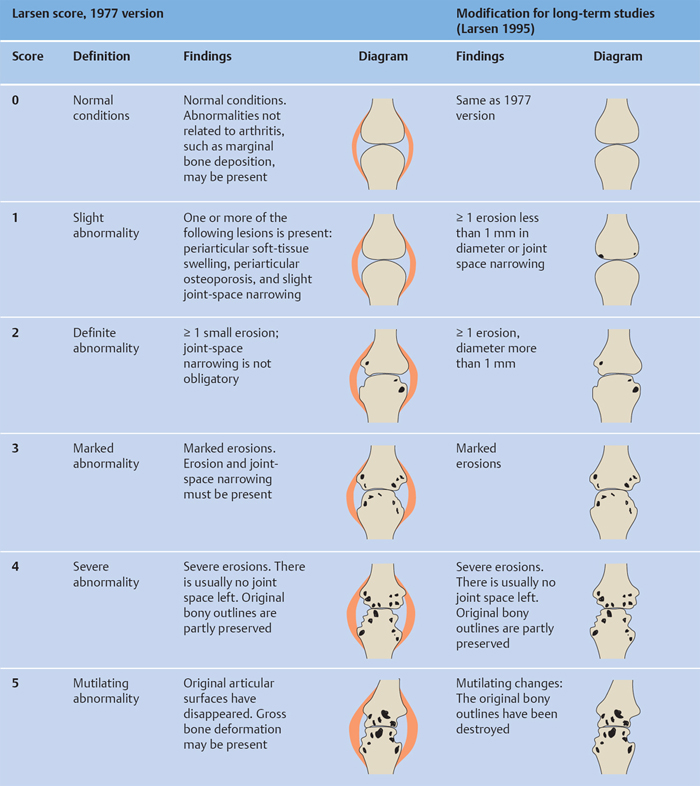
The original 1977 version of the Larsen scoring system focused mainly on erosive destruction. The severity of changes is graded on a 0–5 scale as shown in Fig. 15.1 .
The definitions in the Larsen score relate mainly to radiographic changes of the hands and feet. The following joints are evaluated in the standard protocol:
Second through fifth proximal interphalangeal joints
First interphalangeal joint (thumb)
First through fifth metacarpophalangeal joints
Wrist
First through fifth metatarsophalangeal joints
A total of 32 joints are scored, and the individual joint scores are added together to give a total score between 0 and 160. Originally the different grades of severity were illustrated by standard reference films, but Larsen later replaced the reference films with schematic drawings (see Fig. 15.1 ).
The method was modified several times by Larsen himself and by other authors, but no change was made in the list of joints that are scored. In 1995 Larsen introduced a modification for long-term studies that addressed the difficulty of scoring soft-tissue swelling and articular osteoporosis because of the variable quality of radiographs. This prompted Larsen to redefine grade 1 (one or more erosions < 1 mm in diameter or joint-space narrowing) and grade 2 (one or more small erosions > 1 mm in diameter) (see Fig. 15.1 ). The following joints are scored in this modification ( Fig. 15.2 ):
Second through fifth proximal interphalangeal joints
Second through fifth metacarpophalangeal joints
Radial and ulnar compartments of the wrist
Radial and ulnar compartments of the carpometacarpal joint
Second through fifth metatarsophalangeal joints
Again, a total of 32 joints are counted to yield a total score between 0 and 160.
Larsen A, Dale K, Eek M. Radiographic evaluation of rheumatoid arthritis and related conditions by standard reference films. Acta Radiol Diagn (Stockh) 1977;18(4):481–491 Larsen A, Thoen J. Hand radiography of 200 patients with rheumatoid arthritis repeated after an interval of one year. Scand J Rheumatol 1987;16(6):395–401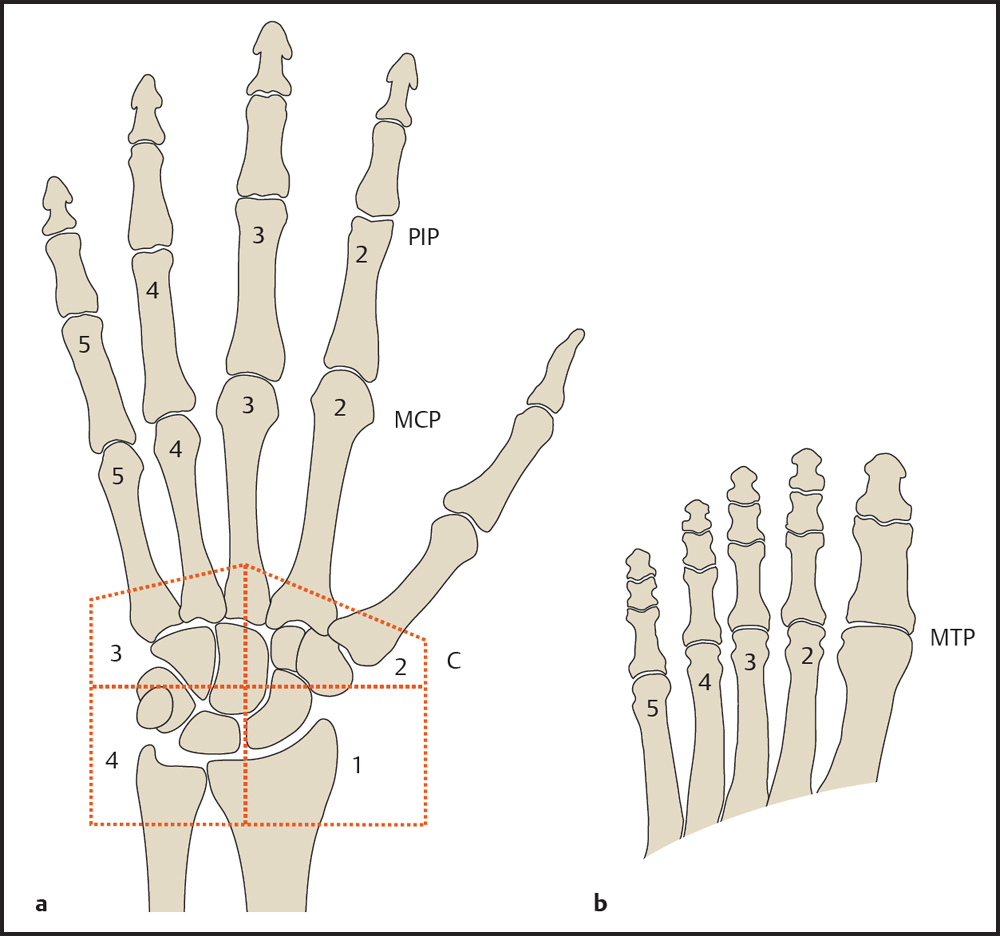
C = Carpus
MCP = Metacarpophalangeal joint
PIP = Proximal interphalangeal joint
b Foot.
MTP = Metatarsophalangeal joint
Larsen A. How to apply Larsen score in evaluating radiographs of rheumatoid arthritis in long-term studies. J Rheumatol 1995;22(10):1974–1975 Rau R, Herborn G, Wassenberg S. Atlas radiologischer Scoringmethoden bei der rheumatoiden Arthritis. Stuttgart: Thieme; 2008
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


