Saber-Sheath Trachea
Aqeel A. Chowdhry, MD
Tan-Lucien H. Mohammed, MD, FCCP
Key Facts
Terminology
Trachea in which coronal dimension ≤ 2/3 of sagittal dimension
Extrathoracic trachea normal
Probably acquired deformity of trachea, usually secondary to chronic obstructive lung disease
Imaging Findings
Normal trachea
Sagittal diameter is 13-27 mm in men and 10-23 mm in women
Coronal diameter is 13-25 mm in men and 10-21 mm in women
Tracheal index (coronal diameter)/(sagittal diameter) usually measured 1 cm above aortic arch
In saber-sheath trachea, tracheal index ≤ 2/3
Specificity for chronic obstructive pulmonary disease (COPD) (95%)
Sensitivity for COPD < 10%
Top Differential Diagnoses
Tracheal Stenosis
Tracheobronchomalacia
Tracheopathia Osteochondroplastica
Amyloidosis
Relapsing Polychondritis
Pathology
Saber-sheath deformity is sign of hyperinflation
Tracheal index correlates with functional residual capacity
May be related to abnormal pattern and magnitude of intrathoracic pressure changes in COPD
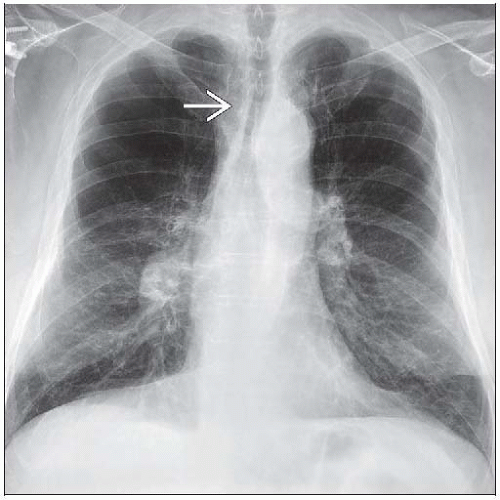 Frontal radiograph shows the typical features of tracheal narrowing  from a saber-sheath trachea. The deformity is often overlooked on chest radiographs. from a saber-sheath trachea. The deformity is often overlooked on chest radiographs. |
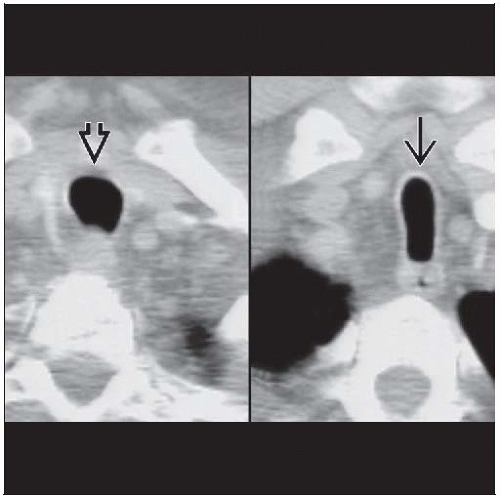 Axial CECT shows a normally shaped extrathoracic trachea  and saber-sheath deformity and saber-sheath deformity  of the intrathoracic trachea. of the intrathoracic trachea. |
TERMINOLOGY
Abbreviations and Synonyms
Tracheal narrowing, tracheomalacia, scabbard deformity
Definitions
Trachea in which coronal dimension is ≤ 2/3 of sagittal dimension
Extrathoracic trachea normal
IMAGING FINDINGS
General Features
Best diagnostic clue
Marked decrease in coronal diameter with increase in sagittal diameter
Inward bowing of lateral tracheal wall usually worsened with forced expiration
Patient position/location
Intrathoracic airway
Main bronchi and extrathoracic trachea are usually normal
Size
Normal trachea
Sagittal diameter is 13-27 mm in men and 10-23 mm in women
Coronal diameter is 13-25 mm in men and 10-21 mm in women
Tracheal index (coronal diameter)/(sagittal diameter) usually measured 1 cm above aortic arch
Round or horseshoe-shaped
Saber-sheath tracheal measurements
Tracheal index ≤ 2/3
Morphology
Saber-sheath deformity
Narrowed trachea on frontal view, widened on lateral view
CT Findings
Morphology
Side-to-side narrowing of trachea at and below thoracic inlet
Tracheal index ≤ 2/3
Specificity for chronic obstructive pulmonary disease (COPD) (95%)
Sensitivity for COPD < 10%
Wall
No tracheal wall thickening
Inner wall of trachea usually smooth
Tracheal cartilage usually calcified
Lung
Hyperinflated, usually from centrilobular emphysema and bullous lung disease
Extrathoracic trachea remains normal in configuration
Tracheal index may increase following lung reduction surgery
Does not return to normal, however
Imaging Recommendations
Best imaging tool: HRCT, as tracheal deformity often overlooked on chest radiographs
Protocol advice: CT during forced expiration or Valsalva maneuver shows inward bowing of tracheal walls
Radiographic Findings
Posteroanterior chest radiograph shows diffuse narrowing of coronal diameter of intrathoracic trachea
Extrathoracic trachea is normal in diameter
DIFFERENTIAL DIAGNOSIS
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


