Clinical Presentation
The patient is a 79-year-old woman who presented with progressive gait disturbance, low back pain, right groin pain, bilateral lower extremity pain, and left shoulder pain. Patient has remote history of breast cancer with prior radiation therapy to the pelvis for previous metastasis, but no objective evidence of tumor recurrence.
Imaging Presentation
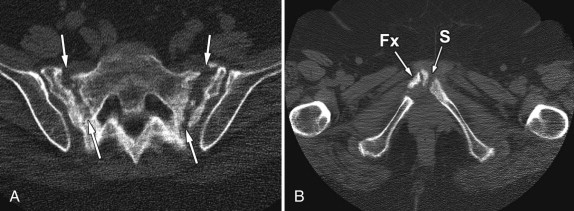
Magnetic resonance (MR) imaging of the lumbosacral spine reveals abnormal signal intensity in both iliac wings consistent with bilateral sacral insufficiency fractures ( Figs. 62-1 and 62-2 ) . Radionuclide bone scan reveals intense bilaterally symmetric uptake in the sacral wings consistent with sacral insufficiency fractures ( Fig. 62-3 ) . Computed tomography (CT) scan of the pelvis reveals fractures of both sacral wings and comminuted fracture to the right of the symphysis pubis ( Fig. 62-4 ) .



Discussion
Sacral stress fractures are estimated to occur in up to 1% of women over 55 years of age. Sacral stress fractures often go undiagnosed clinically because back pain associated with this condition is attributed to other more common conditions of the spine in the elderly. These fractures are also overlooked during image interpretation, especially when the imaging study obtained does not focus specifically on the sacrum. Sacral stress fractures are of two types: (1) Insufficiency fractures are stress fractures of the sacrum resulting from normal stress on abnormal or demineralized bone and (2) fatigue fractures are stress fractures that occur when abnormal or demineralized bone is subjected to abnormal stress. Both types of stress fractures have the same imaging appearance and clinical presentation.
The underlying process responsible for the development of sacral stress fractures is an abnormality of bone mineralization. Many conditions can be associated with abnormal bone density resulting in weakening of the sacrum and other bones. This abnormal “insufficient” bone can be subjected to normal axial loading stress; minor or major trauma or repeated trauma can eventually cause fracture. The most common predisposing condition is osteoporosis, which usually develops in post-menopausal females, so sacral stress fractures are far more common in elderly females. The second most common predisposing condition is post-radiotherapy osteoporosis. Other conditions that predispose to insufficiency fractures include osteomalacia, long-term steroid therapy, renal osteodystrophy, rheumatoid arthritis, Paget’s disease, chronic bed rest, chronic nutritional disorders, and hyperaldosteronism.
Post-menopausal women are most commonly afflicted by sacral stress fractures, but these may also occur in elderly men. Some cases have been reported in pregnant or postpartum women and in long-distance runners. Rarely sacral stress fractures have been reported in the pediatric population, even in nonathletes.
Sacral insufficiency fractures are commonly overlooked initially in the elderly population, the low back pain often being attributed to SI joint arthritis, lumbar spine disc disease, facet arthropathy, or spinal stenosis. Some stress fractures of the sacrum are asymptomatic. However, patients with sacral insufficiency fractures most commonly present with severe low back pain, but also complain of pain in the buttocks, hips, or groin region. The sacrum is often tender to palpation. Radicular symptoms may or may not be present. The back pain is typically worse during activity and usually improves with rest. Rarely, patients with sacral stress fractures present with or develop cauda equina syndrome, which could occur secondary to nerve root traction, nerve root compression, epidural hematoma formation, or perineural inflammation.
Imaging Features
Sacral stress fractures are usually bilateral but can be unilateral. The fractures usually are oriented vertically within the sacral wings but may involve the sacral vertebral bodies, especially in the midsacral region. Occasionally the stress fracture involves only the lower portion of the sacrum. When a sacral stress fracture is discovered, the thoracolumbar spine and other portions of the pelvis should be imaged to rule out other insufficiency fractures. In the pelvis, stress fractures also occur in the pubic rami and in the supra-acetabular region.
Sacral stress fractures may or may not be visible on radiographs of the pelvis as vague vertical regions of increased bone density (sclerosis) in the sacral wings (ala). Normal radiographs of the sacrum do not exclude the presence of sacral insufficiency fractures. Bowel gas frequently obscures the sacrum rendering subtle fractures difficult to visualize. Vertically oriented fracture lines through the sacral ala may be visible on radiographs, but this is not common. Rarely, cortical disruption of the sacral foraminal roofs is visible, but this finding is more commonly observed with traumatic sacral fractures. Radiographs of the spine and pelvis may show other insufficiency fractures.
With CT, vertically oriented fracture lines, if present, are more readily seen ( Figs. 62-5 and 62-6 ) . The sacrum is optimally scanned with thin section helical imaging so reformatted oblique coronal images can be generated, which often display the fracture lines optimally. The fracture lines usually extend through the anterior and posterior cortex, although occasionally the anterior or posterior sacral cortex is spared. As the fracture heals, broad regions of heterogeneous sclerosis form in the sacral wings adjacent to the fracture lines (see Fig. 62-5 ), and the sclerosis may partially obscure the fractures (see Fig. 62-6 ).


Sacral stress fractures are often diagnosed in patients with low back pain undergoing lumbar MR imaging. However, occasionally the sacral insufficiency goes undetected on routine MR imaging of the lumbar spine if careful attention is not given to examining the sacrum or if one relies on sagittal MR images of the sacrum to make the diagnosis ( Fig. 62-7 ) . Sacral fractures are best demonstrated with dedicated axial or oblique coronal MRI or CT images of the sacrum ( Figs. 62-2 and 62-8 ) . The earliest imaging signs of sacral insufficiency fracture are visible with MR imaging as broad regions of heterogeneous T1 hypointensity and T2 hyperintensity in the sacral wings, which often extend to the sacral cortical margin of the sacroiliac (SI) joints (see Fig. 62-8 ). The signal disturbance is most conspicuous on fat-saturated or short tau inversion recovery (STIR) MR images attributed to presence of bone marrow edema (see Figs. 62-2 and 62-8 ). Sacral insufficiency fractures usually involve the upper portion of the sacral wings, but uncommonly the lower portion of the sacrum may be involved ( Fig. 62-9 ) . Sacral insufficiency fractures are usually bilateral but may be unilateral ( Figs. 62-10 to 62-12 ) . Vertebral insufficiency fractures commonly coexist with sacral insufficiency fractures (see Fig. 62-10 ).










