Examination: Ultrasound of the Shoulder
Date of Study: March 11, 2017
Patient Name: Juan Atkins
Registration Number: 8675309
History: Shoulder pain, evaluate for rotator cuff abnormality
Findings: No evidence of joint effusion. The biceps brachii long head tendon is normal without tendinosis, tear, tenosynovitis, or subluxation/dislocation. The supraspinatus, infraspinatus, subscapularis, and teres minor tendons are also normal. No subacromial-subdeltoid bursal abnormality and no sonographic evidence for subacromial impingement with dynamic maneuvers. The posterior labrum is unremarkable. Additional focused evaluation at site of maximal symptoms was unrevealing.
Impression: Unremarkable ultrasound examination of the shoulder. No rotator cuff abnormality.
Examination: Ultrasound of the Shoulder
Date of Study: March 11, 2017
Patient Name: Chazz Michael Michaels
Registration Number: 8675309
History: Shoulder pain, evaluate for rotator cuff abnormality
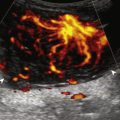
Findings: There is a focal anechoic tear of the anterior, distal aspect of the supraspinatus tendon measuring 1 cm short axis by 1.5 cm long axis. The anterior margin of the tear is adjacent to the rotator interval. There is no involvement of the subscapularis, infraspinatus, or rotator interval. A moderate amount of infraspinatus and supraspinatus fatty degeneration is present. There is a small joint effusion distending the biceps brachii tendon sheath and moderate distention of the subacromial-subdeltoid bursa. No biceps brachii long head tendon abnormality and no subluxation/dislocation. Mild osteoarthritis of the acromioclavicular joint. Additional focused evaluation at site of maximal symptoms was unrevealing.
Impression: Focal or incomplete full-thickness tear of the supraspinatus tendon with infraspinatus and supraspinatus muscle atrophy.
Examination: Ultrasound of the Elbow
Date of Study: March 11, 2011
Patient Name: Kevin Saunderson
Registration Number: 8675309
History: Elbow pain, evaluate for tendon abnormality
Findings: No evidence of joint effusion or synovial process. The biceps brachii and brachialis are normal. The common flexor and extensor tendons are also normal. No significant triceps brachii abnormality. The anterior bundle of the ulnar collateral ligament and lateral collateral ligament complex are normal. The ulnar nerve, radial nerve, and median nerve at the elbow are unremarkable. No abnormality in the cubital tunnel region with dynamic imaging. Additional focused evaluation at site of maximal symptoms was unrevealing.
Impression: Unremarkable ultrasound examination of the elbow.
Examination: Ultrasound of the Elbow
Date of Study: March 11, 2011
Patient Name: Ricky Bobby
Registration Number: 8675309
History: Elbow pain, evaluate for tendon abnormality
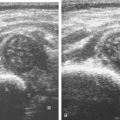
Findings: There is a partial-thickness tear of the distal biceps brachii tendon involving the superficial short head tendon with approximately 2 cm of retraction but with intact long head. Dynamic evaluation shows continuity of the long head excluding full-thickness tear. No joint effusion. The triceps brachii, common extensor, and common flexor tendons are normal. The ulnar, radial, and median nerves are unremarkable, including dynamic evaluation of the ulnar nerve. Unremarkable ulnar and lateral collateral ligaments. No bursal distention.
Impression: Partial-thickness tear of the distal biceps brachii tendon.
Examination: Ultrasound of the Wrist
Date of Study: March 11, 2011
Patient Name: Derrick May
Registration Number: 8675309
History: Numbness, evaluate for carpal tunnel syndrome
Findings: The median nerve is unremarkable in appearance, measuring 8 mm 2 at the wrist crease and 7 mm 2 at the pronator quadratus. No evidence of tenosynovitis. The radiocarpal, midcarpal, and distal radioulnar joints are normal without effusion or synovial hypertrophy. The wrist tendons are normal without tear or tenosynovitis. Normal dorsal component of the scapholunate ligament. No dorsal or volar ganglion cyst. Unremarkable Guyon canal. Additional focused evaluation at site of maximal symptoms was unrevealing.
Impression: Unremarkable ultrasound examination of the wrist.
Examination: Ultrasound of the Wrist
Date of Study: March 11, 2011
Patient Name: Jacobim Mugatu
Registration Number: 8675309
History: Numbness, evaluate for carpal tunnel syndrome
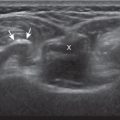
Findings: The median nerve is hypoechoic and enlarged, measuring 15 mm 2 at the wrist crease and 7 mm 2 at the pronator quadratus. No evidence for tenosynovitis. The radiocarpal, midcarpal, and distal radioulnar joints are normal without effusion or synovial hypertrophy. The wrist tendons are normal without tear or tenosynovitis. Normal dorsal component of the scapholunate ligament. No dorsal ganglion cyst. A 7-mm volar ganglion cyst is noted between the radial artery and flexor carpi radialis tendon. Unremarkable Guyon canal. Additional focused evaluation at site of maximal symptoms was unrevealing.
Impression:
- 1.
Ultrasound findings compatible with carpal tunnel syndrome.
- 2.
A 7-mm volar ganglion cyst.
- 1.
Examination: Ultrasound of the Right Hip
Date of Study: March 11, 2016
Patient Name: Jack White
Registration Number: 8675309
History: Hip pain, evaluate for bursitis
Findings: The hip joint is normal without effusion or synovial hypertrophy. Limited evaluation of the anterior labrum is unremarkable. No evidence of iliopsoas bursal distention or snapping iliopsoas tendon with dynamic imaging. The remaining anterior tendons, including the rectus femoris and sartorius, as well as the adductors, are normal.
Evaluation of the lateral hip is normal. No evidence of abnormal bursal distention around the greater trochanter. The gluteus minimus and medius tendons are normal. No abnormal snapping with dynamic evaluation.
Impression: Unremarkable ultrasound examination of the hip.
Examination: Ultrasound of the Right Hip
Date of Study: March 11, 2016
Patient Name: Brennan Huff
Registration Number: 8675309
History: Hip pain, evaluate for tendon tear
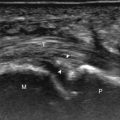
Findings: There is a partial tear of the adductor longus origin at the pubis. No evidence of full-thickness tear or tendon retraction. The common aponeurosis and rectus abdominis tendon are normal, as is the pubic symphysis.
The hip joint is normal without effusion or synovial hypertrophy. There is a possible tear of the anterior labrum. No paralabral cyst. No evidence of iliopsoas bursal distention or snapping iliopsoas tendon with dynamic imaging.
Evaluation of the lateral hip is normal. No evidence of abnormal bursal distention around the greater trochanter. The gluteus minimus and medius tendons are normal. No abnormal snapping with dynamic evaluation.
Impression:
- 1.
Partial-thickness tear of the proximal adductor longus.
- 2.
Possible anterior labral tear. Consider MR arthrography if indicated.
- 1.
Examination: Ultrasound of the Right Knee
Date of Study: March 11, 2016
Patient Name: Meg White
Registration Number: 8675309
History: Trauma
Findings: The extensor mechanism, including the quadriceps tendon, patella, and patellar tendon, is normal without bursal abnormalities. No significant joint effusion or synovial hypertrophy. The medial collateral and lateral collateral ligaments are normal. Unremarkable iliotibial tract, biceps femoris, popliteus tendon, and common peroneal nerve. No Baker cyst. Limited evaluation of the menisci is unremarkable.
Impression: Unremarkable ultrasound examination of the right knee.
Examination: Ultrasound of the Right Knee
Date of Study: March 11, 2016
Patient Name: Frank Ricard
Registration Number: 8675309
History: Pain, evaluate for cyst
Findings: The extensor mechanism, including the quadriceps tendon, patella, and patellar tendon, is normal. There is a moderate-sized joint effusion and no synovial hypertrophy or intra-articular body. The medial and lateral collateral ligaments are normal, as is the iliotibial tract, biceps femoris, popliteus tendon, and common peroneal nerve. There is medial compartment joint space narrowing and osteophyte formation with mild extrusion of the body of the medial meniscus, which is abnormally hypoechoic. No parameniscal cyst. There is a Baker cyst measuring 2 × 2 × 6 cm. Abnormal hypoechogenicity is noted at the inferior margin of the Baker cyst. There is also a hypoechoic cleft involving the posterior horn of the medial meniscus, which extends to the articular surface.
Impression:
- 1.
Baker cyst with evidence for rupture.
- 2.
Medial compartment osteoarthritis with moderate joint effusion.
- 3.
Suspect posterior horn medial meniscal tear. Consider MRI for confirmation if indicated.
- 1.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


