Scaphoid Fracture
Ami V. Vakharia
Daniel B. Nissman
CLINICAL HISTORY
26-year-old fell on an outstretched hand.
 FIGURE 84A |
 FIGURE 84B |
 FIGURE 84C |
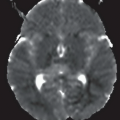
 FIGURE 84D |
FINDINGS
An ulnar-deviated PA radiograph of the left wrist (Fig. 84A) demonstrates an oblique, nondisplaced fracture of the proximal scaphoid pole. A clenched-fist PA radiograph of the right wrist in a second patient (Fig. 84B) demonstrates a transverse, nondisplaced fracture of the scaphoid waist. In a third patient, indeterminate wrist radiographs, represented here by an ulnar-deviated PA view (Fig. 84C), revealed mixed sclerosis and possible lucency in the mid and proximal scaphoid. Subsequent MRI of the wrist, represented here by a coronal T1-weighted image (Fig. 84D), reveals a near-transverse complete fracture of the proximal scaphoid pole and extensive bone marrow edema localized to the scaphoid.
DIFFERENTIAL DIAGNOSIS
Radial styloid fracture, scaphoid fracture, lunate dislocation.
DIAGNOSIS
Scaphoid fracture.
DISCUSSION
Scaphoid fractures most commonly occur in active young people, typically males in their 20s, and account for the majority of carpal bone fractures. Scaphoid fractures are frequently associated with a fall on an outstretched hand that result in forced dorsiflexion of the wrist. In this position, the scaphoid becomes trapped against the dorsal lip of the distal radius while being held in place by the strong ligamentous support of the scaphoid leading to high tensile stress on the concave volar aspect of the scaphoid. The most common location of scaphoid fractures in descending order is the waist, proximal pole, distal pole, and the tubercle (distal volar prominence). Symptoms commonly include radial wrist pain (“anatomic snuff box pain”) with minimal swelling and possible decreased range of motion.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


