Figure 5-38. The two constant bursae at the STJ. Schematic drawing of a superior view of the left shoulder. The supraserratus bursa (ssb) is located between the serratus anterior (sa) and subscapularis muscles (sub), whereas the infraserratus bursa (isb) is located between the serratus anterior and the thoracic cage (rib). Pm= pectoralis major muscle. Hum= humerus. Sca= scapula.
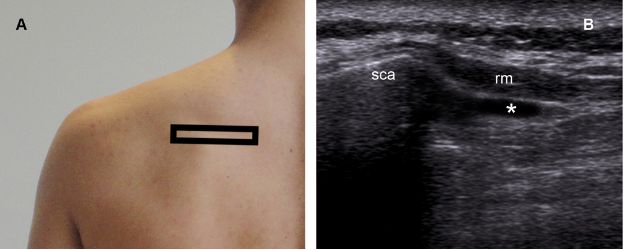
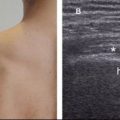
Figure 5-39. Infraserratus bursitis. [A] Positioning of the probe. [B] Corresponding 12-5 MHz US image shows fluid distension of the infraserratus bursa (asterisk), which provides a low-friction surface to facilitate rotation of the scapula (sca). Rm= rhomboid minor.
Muscular abnormalities associated to snapping scapula include atrophy and anomalous muscle insertions. Postoperative unilateral atrophy of the serratus anterior muscle is not uncommon following anterolateral thoracotomy with posterior extension and is considered the classical example of muscular abnormalities related to snapping scapula (figure 5-40). Clinical and experimental studies suggest stretching or sectioning of long thoracic nerve as the most likely cause.96
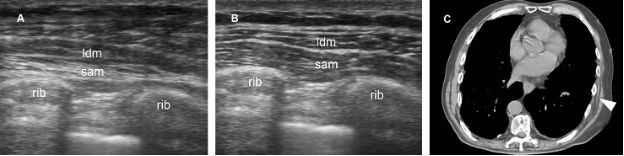
Figure 5-40. Unilateral atrophy of the serratus anterior muscle. [A] Axial 12-5 MHz US image obtained from the left thoracic wall shows decreased volume and increased echogenicity of the serratus anterior muscle (sam). [B] Comparative 12-5 MHz US image obtained from the right thoracic wall shows normal serratus anterior muscle. [C] Corresponding CT confirms sonographic finding of left atrophy (arrowhead). Ldm= latissimus dorsi muscle. Rib= rib.
Another soft-tissue cause for snapping scapula is elastofibroma dorsi, a benign reactive fibroelastic hyperproliferation first described by Jarvi and Saxen in 1961.97 The typical presentation involves a slow-growing periscapular mass that almost exclusively affects individuals over the age of 40, with sporadic cases arising in children and adolescents.98,99 The lesion is believed to result from repeated mechanical friction between the thoracic wall and the inferior angle of the scapula. However, it may also result as a natural consequence of aging, rather than abnormal elastogenesis or degeneration. Large case series from Japan strongly suggest familial predisposition.100,101 At US, elastofibromas are depicted deep to the musculature as a multilayered pattern of hypoechoic linear areas of fat deposition intermixed with echogenic fibroelastic tissue (figure 5-41).102 The mass often protrudes from the subscapular region upon shoulder abduction, allowing better delineation of the finding.103-105 Elastofibromas can be differentiated from the most common lipoma on the basis of typical location and well-defined multilayered pattern.100 Complete surgical excision is the treatment of choice in symptomatic patients.
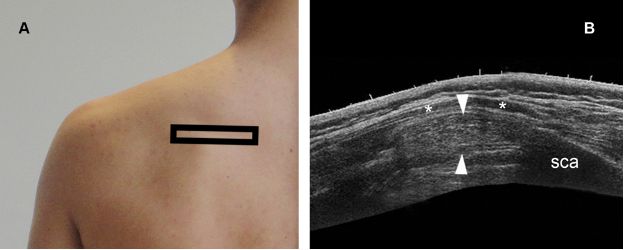
Figure 5-41. Elastofibroma dorsi. [A] Positioning of the probe. [B] Corresponding extended field of view 12-5 MHz US image shows a typical echogenic fibroelastic mass (arrowheads) located deep to the trapezius muscle (asterisks). Sca= scapula.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


