Screening
Apocrine carcinomas
Artifacts
Axillary nodal metastasis
Batch interpretation
Biopsy changes
Breast cancer statistics
Call-back (recall) rates
Contrast
Craniocaudal views (CC)
Cysts
Diffuse changes
Distortion
Ductal carcinoma in situ (DCIS)
Exaggerated craniocaudal views laterally (XCCL)
Exposure
Fibroadenoma
Focal parenchymal asymmetry
Global parenchymal asymmetry
Invasive ductal carcinoma, not otherwise specified (NOS)
Invasive lobular carcinoma
Isolated tumor cells
Kilovoltage peak (kVp)
Lymphovascular space involvement
Mediolateral oblique views (MLO)
Micrometastasis
Milliamperage output (mAs)
Mondor disease
Ninety-degree lateromedial views (LM)
Ninety-degree mediolateral views (ML)
Poland syndrome
Posterior nipple line (PNL)
Reduction mammoplasty
Quantum mottle
Shrinking breast
Screening guidelines
Screening views
Sharpness
Triangulation
Mammography can demonstrate clinically occult breast cancers. Is this significant? Does this make a difference? Does finding clinically occult cancers affect overall mortality from breast cancer? Yes, yes, and yes. Support for the routine use of screening mammography is provided by results from seven of eight randomized controlled trials in large populations of women, including 40- to 49-year-old women. These studies demonstrated a 20% to 32% reduction in breast cancer mortality among the women invited to undergo screening mammography. Updates from the two-county Swedish trial have reported 20-year survivals of 87.3% and 83.8% among women identified with tumors <0.9 cm and 1.0 to 1.4 cm in size, respectively. The goal of screening mammography (and our job), therefore, is to consistently identify breast cancers that are <1.4 cm (ideally, <0.9 cm). It is noteworthy that the most common method of breast cancer detection is now screening mammography (as opposed to breast self-examination), and that mortality rates from breast cancer continue to drop.
Based on the scientific evidence and expert opinion available, an independent panel of 42 medical and scientific experts developed new breast cancer screening guidelines that were adopted and published by the American Cancer Society (ACS) in 2003. The ACS recommends annual screening mammography starting at age 40 years and continuing for as long as a woman is in good health. Clinical breast exams should be part of a periodic health exam about every 3 years for women in their 20s and 30s and annually for women aged 40 years and older. Women should report any breast change they detect promptly to their health care provider. Beginning in their 20s, women should be told about the benefits and limitations of breast self-examination (BSE). It is acceptable for women to choose not to do BSE or to do it only occasionally. Women known to be at increased risk (e.g., personal or strong family history of breast cancer, a genetic tendency or prior mediastinal radiation therapy for Hodgkin lymphoma) may benefit from earlier initiation of early-detection testing, screening at shorter intervals, and/or the addition of breast ultrasound or magnetic resonance imaging (MRI). Indeed, since 2003, several reports have supported the use of MRI for the detection of small cancers in high-risk women.
It was estimated that 211,240 new cases of breast cancer would occur in 2005 among women in the United States. Among men, 1,690 new breast cancer cases were expected in 2005. The estimated
numbers of deaths resulting from breast cancer in 2005 among women and men were 40,410 and 460, respectively. A decline in the mortality rate from breast cancer of 2.3% per year from 1990 to 2000 has been reported among all women, with larger decreases in women under age 50 years. The decline in the mortality rate is attributed to earlier detection and improved treatment.
numbers of deaths resulting from breast cancer in 2005 among women and men were 40,410 and 460, respectively. A decline in the mortality rate from breast cancer of 2.3% per year from 1990 to 2000 has been reported among all women, with larger decreases in women under age 50 years. The decline in the mortality rate is attributed to earlier detection and improved treatment.
Craniocaudal (CC) and mediolateral oblique (MLO) views are the standard screening views. In addition to routine views, our technologists obtain anterior compression and exaggerated craniocaudal (XCCL) views, as needed, to tailor the screening study to the individual woman.
Compared to online reading, batch interpretation of screening mammograms is cost-effective and efficient. With batch interpretation, the patient leaves the imaging facility after her routine views are done and reviewed by the technologist for technical adequacy. The mammograms are hung on high-luminance, dedicated mammography multiviewers for interpretation by the radiologist at a later time. At our facility, right and left CC and right and left MLO views are hung back to back. The two CC views are placed side by side with the two MLO views. If they are available, films from 2 years before are hung above the current study for comparison. Subtle changes may not be apparent from one year to the next, but may be more easily perceived if a study other than the one from 1 year ago is used for comparison. However, before calling a patient back for a diagnostic study, reviewing the mammogram from the year before is often helpful to make sure the current area of concern was not evaluated last year. Any additional studies done at our center are kept in jackets close to the multiviewer so that they can be reviewed as deemed necessary by the interpreting radiologist.
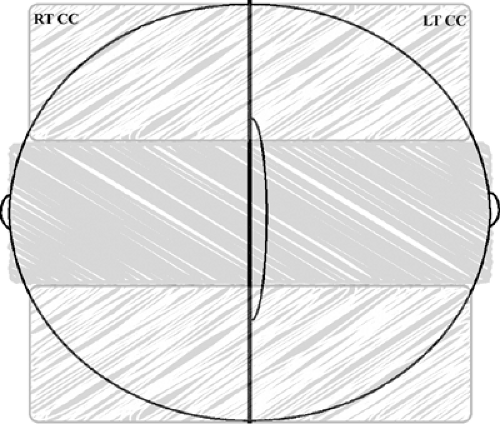 Figure 2.1. Image evaluation. On craniocaudal views, narrow the search for potential lesions by splitting the images in thirds. This will help you to focus attention on smaller amounts of tissue. Go back and forth between the right and left craniocaudal views, looking specifically for asymmetries, possible masses, distortion, or calcifications. |
In evaluating screening mammograms, I recommend developing a viewing strategy that is systematic and is used consistently. I also think it is important to have a proactive and focused mindset when reviewing studies, rather than waiting passively for more subtle findings to become apparent. In other words, send your eyes out looking for potential lesions in specific locations; otherwise you may miss subtle findings or study limitations (e.g., blurring) that may preclude detection of possible abnormalities. Chance favors a prepared mind. Ideal viewing conditions are equally important. All extraneous light should be eliminated so that the only light in the room is coming through the films being reviewed. Paper work and interruptions should be minimized.
Whatever approach you use, it should begin with a review of the films for technical adequacy. Specifically, is positioning acceptable? Has any tissue, and possibly a lesion, been excluded from the films (e.g., do you see tissue at the edge of any of the films)? Is glandular tissue adequately compressed and penetrated (exposed)? Are the films high in contrast? Are there any artifacts that may preclude adequate interpretation? Is there any blurring?
Look for diffuse changes that may be difficult to perceive, particularly if you are focused on detecting smaller potential lesions. Is one breast larger or more dense than the other? Don’t assume that the larger breast is the abnormal breast; the smaller breast may be progressively “shrinking.” Are the technical factors needed for adequate exposure of one breast significantly different from those used to expose the contralateral side? Is compression limited (e.g., centimeters of compression or decanewtons used)? Is there prominence of the trabecular markings? Do you see trabecular markings superimposed on the pectoral muscles (e.g., reminiscent of “kerley” B lines)? Are there any findings in the axillary regions?
After evaluating the mammogram globally for technical adequacy and diffuse changes, look specifically both with and without a magnification lens for masses, areas of asymmetry, architectural distortion, and calcifications. Narrowing the search is helpful in focusing your review. On CC views, look at the lateral, middle, and medial thirds of the breasts (Fig. 2.1). On MLO views, evaluate the
upper, middle, and lower thirds of the breasts (Fig. 2.2). Search out potentially abnormal areas as you go back and forth between the right and left breasts. Also, evaluate fat–glandular interfaces specifically for straight lines or convex tissue bulges, the fatty stripe of tissue between the pectoral muscle and glandular tissue on MLO views, the superior cone of tissue on MLO views, the subareolar areas, and the medial portions of the breasts on CC views (Fig. 2.3).
upper, middle, and lower thirds of the breasts (Fig. 2.2). Search out potentially abnormal areas as you go back and forth between the right and left breasts. Also, evaluate fat–glandular interfaces specifically for straight lines or convex tissue bulges, the fatty stripe of tissue between the pectoral muscle and glandular tissue on MLO views, the superior cone of tissue on MLO views, the subareolar areas, and the medial portions of the breasts on CC views (Fig. 2.3).
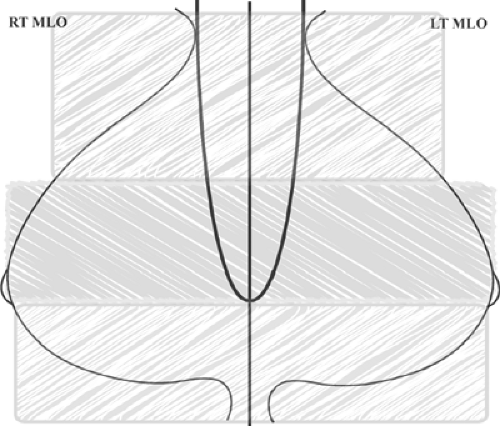 Figure 2.2. Image evaluation. On mediolateral oblique views, narrow the search for potential lesions by splitting the images in thirds. This will help you to focus attention on smaller amounts of tissue. Go back and forth between the right and left mediolateral oblique views, looking specifically for asymmetries, possible masses, distortion, or calcifications. |
After formulating a working hypothesis on a given mammogram, compare it with prior studies and look at the history form for potentially relevant factors (hormone replacement therapy, prior breast surgery, family history of breast cancer, skin lesions etc.). Be careful not to let prior films influence decisions regarding the relevance of a finding on the current study. In some women, it is important to look at several comparison studies. If you perceive an area of spiculation or distortion that cannot be explained by a history of surgery, trauma, or mastitis at that specific site, the patient should be evaluated in spite of apparent stability. Stability of a lesion does not assure that it is benign.
Make no assumptions. If you assume something is benign or malignant, it becomes very difficult to think otherwise. Also, if there is an obvious finding, make a conscientious effort to look at the remainder of the mammogram first. Do not focus your attention on obvious findings to the exclusion of other subtle, and potentially more significant, findings.
On screening studies, my goal is to detect potential abnormalities. I make no particular effort to characterize potential or true lesions on screening studies. Over the years it has become apparent to me that sometimes what I think is a significant lesion on the screening mammogram turns out to be insignificant after additional evaluation and what I initially think is almost certainly benign is cancer. Similarly, in some patients, what is seen on the screening studies turns out to represent a more extensive lesion (“the tip of the iceberg”). Why make decisions with insufficient and potentially misleading information? Why work with low confidence? Additional evaluation increases certainty in making appropriate recommendations and narrows differential considerations to one or two options. Recommendations are more easily justified following complete and thorough evaluations. With the confidence generated by the additional evaluation, succinct, definitive, and directive reports can be generated.
For women with an obvious lesion on the screening study, additional evaluation helps characterize the extent of the lesion and sometimes establishes the presence of other, initially unsuspected, lesions. It provides an opportunity to communicate directly with the patient and undertake imaging-guided biopsies at the time of call-back. In essence, we expedite patient care. Consequently, the only BI-RADS® assessment categories I use on screening studies are category 1 (negative), category 2 (benign finding), and category 0 (needs additional imaging evaluation or needs prior mammograms for comparison).
Category 0 is used when additional studies are indicated or when prior studies are to be requested and comparison is needed to make a final assessment. For those women in whom a potential abnormality is detected, we categorize the call-back as level 1, 2, or 3. These levels are used internally to indicate the amount of time that should be allotted for the patient’s diagnostic appointment. Fifteen, thirty, and sixty minutes are allowed for level 1, 2, and 3 call-backs, respectively. In general, level 1 designates those patients for whom physical examination, additional mammographic images, or an ultrasound are all that should be needed to resolve the question. If the interpreting radiologist expects that a patient will need additional mammographic images and an ultrasound, the call-back is designated as level 2. When the radiologist expects that the patient will need a biopsy, level 3 is used so that an adequate amount of time is
available to do a biopsy when the patient returns for additional evaluation. Although this is an arbitrary classification, characterized by times when, after completing the evaluation, a level 1 call-back patient requires a biopsy and a level 3 call-back patient does not, the system works well. It provides for more efficient use of the schedule and allows us to complete evaluations in one visit. It has enabled us to optimize patient care in a practical and cost-effective manner.
available to do a biopsy when the patient returns for additional evaluation. Although this is an arbitrary classification, characterized by times when, after completing the evaluation, a level 1 call-back patient requires a biopsy and a level 3 call-back patient does not, the system works well. It provides for more efficient use of the schedule and allows us to complete evaluations in one visit. It has enabled us to optimize patient care in a practical and cost-effective manner.
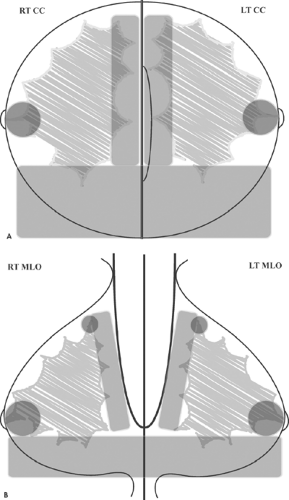 Figure 2.3. Image evaluation. A: On the craniocaudal views, evaluate areas where breast cancers are likely to develop—specifically, the medial quadrants, subareolar areas, fat-glandular interfaces, and the retroglandular areas posteriorly. B: On the mediolateral oblique views, evaluate areas where breast cancers are likely to develop—specifically, the fatty stripe of tissue between the pectoral muscle and glandular tissue, the superior cone of tissue, subareolar areas, and the inferior aspects of the breasts. |
At the time of the screening study, the technologist informs the patient about the possibility of a call-back for further evaluation. In addition, each woman is given a written statement that describes the process for reviewing her mammogram, issuing a report to her doctor, sending her a letter with results, and the possibility of being called back for a diagnostic evaluation. It is important for women to be informed of the process and to know that being called back does not necessarily mean they have cancer. Our goal is to minimize some of the anxiety experienced by patients when they are called back for additional evaluation. It does not always work, but it does help some women.
All women who require additional evaluation are contacted directly by a member of our staff. By communicating with the
patient directly, we can explain the reason for the call-back more appropriately than others might (e.g., as opposed to having a referring physician’s office tell the patient that the first images taken were no good), and we reassure the patient regarding the need for additional studies. This method also expedites patient care by decreasing the amount of time needed to schedule the diagnostic evaluation. If we are unable to contact the woman by phone within 48 hours following her screening study, we send a letter via regular mail asking her to call us. If after a week from mailing the letter we still have not heard from the patient, a certified letter is mailed to her with a copy to the referring physician. All efforts to communicate with the patient are documented in her chart.
patient directly, we can explain the reason for the call-back more appropriately than others might (e.g., as opposed to having a referring physician’s office tell the patient that the first images taken were no good), and we reassure the patient regarding the need for additional studies. This method also expedites patient care by decreasing the amount of time needed to schedule the diagnostic evaluation. If we are unable to contact the woman by phone within 48 hours following her screening study, we send a letter via regular mail asking her to call us. If after a week from mailing the letter we still have not heard from the patient, a certified letter is mailed to her with a copy to the referring physician. All efforts to communicate with the patient are documented in her chart.
A report is generated for all studies in which a prior mammogram is requested and comparison is needed to make a final assessment. These reports are assigned to a category “0”; we do not keep undictated studies aside pending arrival of comparison films. By generating a report, the referring physician is informed that we are working on obtaining prior studies and a system to track the patient is set in motion that minimizes the likelihood of a patient “falling through the cracks.” We allow a 2-week interval during which we make every effort to locate prior studies; this includes calling the facility indicated by the patient on her history form. If this action is unsuccessful, we contact the referring physician and request prior mammogram reports that will indicate the name of the facility and the date of the prior study. Lastly, we sometimes call the patient to verify the information she provided. If we are unable to obtain prior films after 2 weeks, an addendum to the initial report is issued and we dictate the findings as though there were no prior studies. Every effort we make to procure prior studies is documented in the patient’s file.
What is an appropriate call-back (recall) rate? This is an important question to consider and is something radiologists involved in screening mammography should monitor routinely. Calling a patient back for diagnostic evaluation is not innocuous and should never be trivialized. In some women, it is associated with significant morbidity that at times is (unfortunately) grossly underestimated. Regardless of how much you try to prepare a woman for the possibility of a call-back, it is guaranteed to provoke anxiety and stress in most women. High recall rates are also associated with increased costs and decreased efficiency of screening programs. Counter this with our goal of never missing an opportunity to diagnose an early breast cancer. Undoubtedly, to call back or not is a fine line that needs to be considered carefully. Depending on the availability of prior films, you can expect call-back rates to be higher among women with no prior studies compared to those women in whom prior films are available. In considering the call-back rate for individual radiologists, I think it is important not to consider this a static figure but rather a work in progress. Early in the career of a radiologist one should expect and accept higher call-back rates. However, the rate should decrease progressively with the number of screening mammograms evaluated over time. Although it is inconvenient and not usually easy to schedule, the ideal learning situation is for the radiologist recommending the call-back to be the one involved in the diagnostic workup. Under these circumstances, meaningful call-back rates can be generated and improvement shown over the years. It is also important to recognize that most call-backs for diagnostic evaluations do not lead to biopsies. Based on published reports, the American College of Radiology recommends that call-backs be maintained at a rate of 10% or less.
In this chapter, the screening mammogram is the starting point for all patients discussed. Focus your attention initially on systematically reviewing the images as described above. Determine if the mammogram is normal or potentially abnormal. Some differentials are included, and pathology results are provided for those patients for whom biopsy is appropriate. I also need to state the obvious at the onset of this chapter: What I present is an artificial situation. For didactic purposes, I have presented a significant number of patients with breast cancer in this chapter; in a true screening program, most of the mammograms you review are normal.
Patient 1
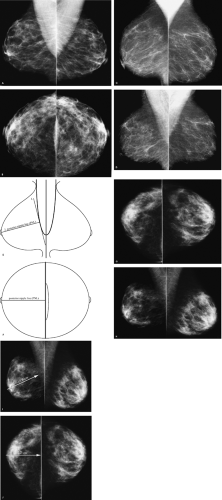 Figure 2.4. Screening studies. Mediolateral oblique (A) and craniocaudal (B) views. Mediolateral oblique (C) views with suboptimal positioning. Although the pectoral muscles are thick at the axilla, the anterior margins are not convex and they do not extend to the level of the nipple. The shape of the muscles is triangular. Repeat mediolateral oblique (D) views, using optimal technique, show thick pectoral muscles at the axilla with convex anterior margins extending to the level of the nipples. Posterior nipple line. E: The posterior nipple line (PNL) is measured when it is suspected that posterior tissue is excluded on a craniocaudal (CC) view. It is most useful when positioning on the corresponding mediolateral oblique view is optimal. A line (1) can be drawn to delineate the anterior margin of the pectoral muscle. The PNL (2) is a perpendicular line drawn from the nipple to the anterior edge of the pectoral muscle. The PNL is measured. This measurement provides an estimate of the amount of tissue that should be included on the CC views. F: On the CC view, the PNL extends from the nipple to the edge of the film. The measurement of the PNL on the CC view should be within 1 cm of that measured on the MLO view. Craniocaudal (G) and mediolateral oblique (H) views. Mediolateral oblique (I) and craniocaudal (J) views showing the posterior nipple line measurements. An inadequate amount of tissue is included on the right craniocaudal view. Repeat right craniocaudal (K) view. Fat is now seen at the edge of the film. Repeat right craniocaudal (L) view with the posterior nipple line measuring 10 cm, which is comparable to that measured on the original mediolateral oblique view. |
In assessing images for technical adequacy, what factors should you evaluate?
The technical factors you should evaluate before focusing on potential abnormalities include positioning, compression, exposure, contrast, sharpness, noise, artifacts, and film labeling. As an interpreting radiologist, you are the gatekeeper for image quality and overall patient care at your facility. If you are willing to routinely interpret suboptimal studies without a good explanation that is well documented (a patient with Parkinson’s disease, a frozen shoulder, history of stroke, etc.), you are basically willing to accept a potential delay in the diagnosis of breast cancer. The overall quality bar at your facility will be as high as you set it.
In evaluating positioning on mediolateral oblique (MLO) views, the pectoral muscles should be wide in the axillary regions, extend to the level of the nipples, and have convex margins anteriorly. The breast needs to be lifted (e.g., not sagging or drooping) so that the inframammary fold is open and a small amount of upper abdomen is included on the image (Fig. 2.4A). As the technologist positions the breast, she needs to establish the angle of obliquity of the patient’s pectoral muscle; it is easier to mobilize tissue maximally away from the body if it is pulled parallel to underlying muscle fibers. Using the appropriate angle for the patient and having the patient lean in slightly to relax the muscle, the technologist needs to mobilize the breast and muscle medially as much as possible and maintain the medial mobilization of the breast as compression is applied and the breast is lifted up and pulled out. If an incorrect angle of obliquity is selected, the breast is not mobilized as much as possible medially, or if the patient moves out of the unit as compression is applied, the pectoral muscle may not be thick at the axilla, extend to the level of the nipple, or it may have a concave margin, a triangular shape, or be parallel to the edge of the film (Fig. 2.4C).
Positioning
In positioning patients for craniocaudal views, the technologist needs to identify the inframammary fold and lift the breast as much as the natural mobility of the breast permits. Next she needs to pull the breast tissue out and actively tug on the lateral aspect of the breast so as to include as much posterolateral tissue as possible. On craniocaudal (CC) views, you should expect to see pectoral muscle in 30% to 40% of patients. When you see pectoral muscles on the CC views, you can be assured that posterior tissue has been included on the images (Fig. 2.4B). If pectoral muscle is not seen on the CC view, look for cleavage as an indication that medial tissue has not been excluded from the image. If no pectoral muscle or cleavage is seen, measure the posterior nipple line (PNL) on the MLO view and compare it with the measurement on the CC view (Fig. 2.4E, F). The measurements should be within 1 cm of each other. Also, evaluate the lateral aspect of the images. If there is tissue extending to the edge of the film, the technologist did not pull lateral tissue in, or an exaggerated craniocaudal view laterally (XCCL) may need to be done to evaluate the patient adequately in the craniocaudal projection.
What are your observations concerning the positioning on this patient’s mammogram?
Retroglandular fat is seen laterally on the left craniocaudal view. Tissue is seen extending to the edge of the film on the right craniocaudal view, and although the right breast is smaller than the left, is there an adequate amount of posterior tissue on the right craniocaudal view? How can you determine this? Measuring the PNL is helpful in assessing if the amount of tissue imaged on the craniocaudal view is adequate (Fig. 2.4I, J). In this patient, the PNL measurement on the right MLO view is 10 cm, compared to 7.2 cm on the right CC view. A significant amount of posterior tissue is excluded from the right CC view and therefore it needs to be repeated. Focusing on technique, a repeat CC view (Fig. 2.4K) is obtained and demonstrates a significantly greater amount of tissue. There is now fat at the edge of the film and the PNL measurement on this second CC view (Fig. 2.4L) is 10 cm, which is equal to what is measured on the MLO view. If images that are missing 2.8 cm of posterior tissue (as on the original right CC view in this patient) are accepted and interpreted, our goal of finding cancers that are less than 1 cm in size is compromised significantly.
In addition to positioning, compression needs to be assessed by specifically evaluating the images for uneven or inadequate exposure, motion blur, and poor separation of parenchymal densities.
Additional Technical Factors to Assess
Glandular tissue needs to be adequately exposed so that there is visualization of trabecula, small tubular structures, and vessels. In many women, adequate penetration of the glandular tissue overexposes the skin and subcutaneous tissue. Image contrast is also important. Ideally, contrast is maximized so that subtle density differences in glandular tissue can be appreciated. Subcutaneous and retroglandular fat is dark gray or nearly black in high-contrast images. Poor-contrast images are characterized by dull gray retroglandular and subcutaneous fat, and the skin is readily apparent.
Sharpness needs to be evaluated by looking specifically for blurring (i.e., unsharpness). The most common cause of blur is patient motion. This is why adequate breast compression is critical. Short exposures (ideally, <2 s) are also helpful in minimizing motion blur. Motion blur does not always involve the entire image. It can be localized to one area on the mammogram, where it is commonly caused by lack of uniformity in breast compression. Poor film screen contact can also be a cause of localized unsharpness. Sharpness is also affected by focal spot size, object-to-image distance, and source-to-image distance. Increases in focal spot size
and object-to-image distance as well as decreases in source-to-image distance contribute to geometric unsharpness.
and object-to-image distance as well as decreases in source-to-image distance contribute to geometric unsharpness.
The ability to detect small structures such as calcifications is decreased by noise (e.g., radiographic mottle). Quantum mottle is the major cause of noise in mammography. Noise can be identified on an image by a background density that is not homogeneous and results in loss of sharpness and visualization of low-contrast structures.
Artifacts can result from x-ray equipment (filter, compression paddle, image receptor holder, grid, etc.), patient factors (deodorant, hair, jewelry, tattoos, etc.), and cassette, film, and screen factors (upside-down cassette in bucky, film scratches, dents, fingerprints, pick-off, moisture, incorrect film loading so that the emulsion side is away from the screen, fog, static, foreign objects on the screen, etc.). Ideally, most images are artifact free. Depending on the overall effect on image quality, films with artifacts may need to be repeated.
With respect to film labeling, the following information is required on all films: patient name, unique patient identification number, date of study, radiopaque laterality and projection markers placed closest to the axilla, facility name, facility location (city, state, and Zip code), technologist identification, cassette/screen identification number, and mammography unit identification number if there is more than one unit in the facility.
Patient 2
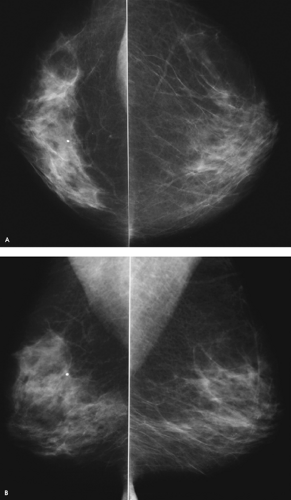 Figure 2.5. Screening study, 43-year-old woman. Craniocaudal (A) and mediolateral oblique (B) views. |
How would you describe the findings on this mammogram?
Compared to the left breast, the right breast is smaller, with dense, asymmetrically distributed tissue (i.e., global parenchymal asymmetry). Although breast size and tissue are commonly symmetric, asymmetries in breast size and tissue distribution can be seen in numerous women as a normal variant. No mass or distortion is noted in the area of increased tissue on the right. The tissue in the right breast is scalloped and contains areas of fatty lobulation. A solitary dense dystrophic calcification is present in the right breast.
What two pieces of information are critical in this patient?
In this woman, it is important to determine that there is no palpable abnormality in the right breast and that the asymmetry in size (either a decrease in size on the right or an increase in size on the left) is not a new or developing change. If they are available, comparison with multiple prior studies is critical, as is a history of prior right breast surgery or trauma. If there is any question about a corresponding palpable abnormality or a progressive change in breast size, the patient can be asked to return for correlative physical examination and, if needed, additional mammographic views, ultrasound, or, occasionally, magnetic resonance imaging. When they are abnormal, asymmetric changes may be the result of chest wall trauma (e.g., burns), congenital abnormalities (e.g., Poland syndrome), or surgery. Invasive ductal carcinomas can present with global areas of parenchymal asymmetry, but these are usually clinically apparent and readily palpable. Invasive lobular carcinoma can also present with global areas of parenchymal asymmetry and progressive changes in breast size (either increases or decreases); palpable findings may be present, but they are often more subtle in patients with invasive lobular carcinomas. Rarely, lymphoma can present with diffuse, asymmetric involvement of one breast.
What do you think about the amount of posterior tissue imaged on the right craniocaudal view?
What BI-RADS® category would you assign?
Are you sure?
Pectoral muscle and retroglandular fat are imaged on the right craniocaudal view and there is no tissue extending to the edge of the film, so it is unlikely that posterior tissue has been excluded from the image.
No change is noted in comparing with multiple prior studies (not shown).
This is categorized as BI-RADS® category 1: negative. BI-RADS® category 2: benign finding can be used if the observations are described in the report. Annual screening mammography is recommended.
Patient 3
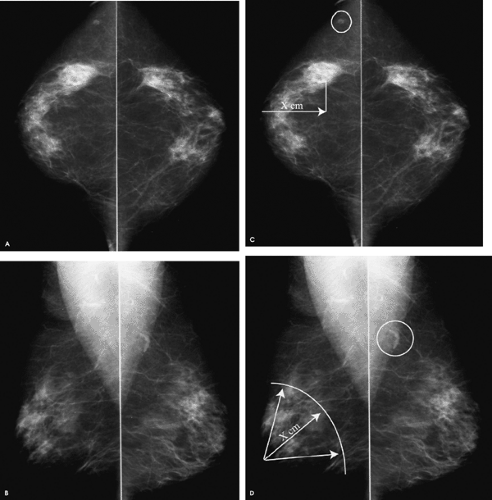 Figure 2.6. Screening study, 81-year-old woman. Craniocaudal (A) and mediolateral oblique (B) views. Craniocaudal (C) and mediolateral oblique (D) views. The distance to the possible lesion is measured from the nipple as “X” cm on the craniocaudal (CC) view. As “X” cm is measured back from the nipple on the mediolateral oblique (MLO) view, an arc can be created that describes the approximate location for the possible lesion noted in the right CC view. No comparably sized area is identified in the MLO view. Intramammary lymph nodes described above are within the circles on the images. |
What do you think of the positioning on the craniocaudal (CC) views?
What BI-RADS® category would you assign, and what is your recommendation?
Patient positioning in this study is acceptable. Although no pectoral muscle is seen on the craniocaudal views, cleavage is seen medially and there is retroglandular fat bilaterally (i.e., no tissue is seen at the edge of the films). A lymph node is noted superimposed on the left pectoral muscle, and one is seen laterally on the right craniocaudal view.
What do you think of the rounded area of asymmetric tissue laterally in the right breast?
Do you see a potential abnormality of comparable size, shape, and density when you evaluate the mediolateral oblique (MLO) view? Based on the location of this area on the CC view, look specifically at where you would expect to find the corresponding area on the MLO view. Using the distance of this area from the nipple on the CC view (Fig. 2.6C), generate an arc on the MLO view (Fig. 2.6D) to help you approximate the expected location of this area on the MLO view.
With the exception of some invasive lobular carcinomas, most breast cancers are three-dimensional structures with comparably sized and shaped abnormalities on any view of the breast. In this woman, there is no comparable area in size, shape, or density on the MLO view. For potential lesions >1 cm in size noted on one view, a comparable abnormality should be identified on the other projection at approximately the same distance from the nipple.
BI-RADS® category1: negative. Annual screening mammography is recommended.
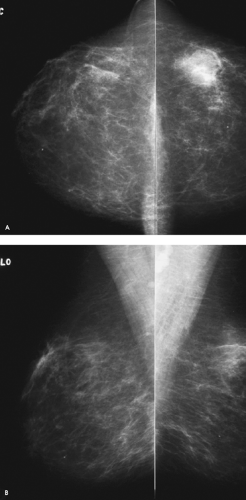 Figure 2.7. Screening study, 45-year-old woman. Craniocaudal (A) and mediolateral oblique (B) views. |
Patient 4
What do you think?
What BI-RADS® category would you assign, and what is your recommendation?
A rounded, asymmetric island of tissue is noted laterally in the left breast. However, in evaluating the mediolateral oblique view, no comparably sized or shaped area is identified that would correspond to the approximate location of this area on the craniocaudal view. Relatively low-density tissue is seen superiorly, characterized by scalloping, interposed fat, and a gradual transition in density. As illustrated here, asymmetric tissue is often planar (i.e., best seen in one projection and changes significantly in appearance on other views), scalloped, heterogeneous in density because of interspersed fat, and characterized by a gradual change in density at the margins. Masses are three-dimensional, with an abrupt change in density and a bulging (convex) margin. True lesions, particularly when >1 cm, are of comparable size, shape and density on the two standard projections and are at approximately the same distance from the nipple on the two views.
BI-RADS® category 1: negative. Annual screening mammography is recommended.
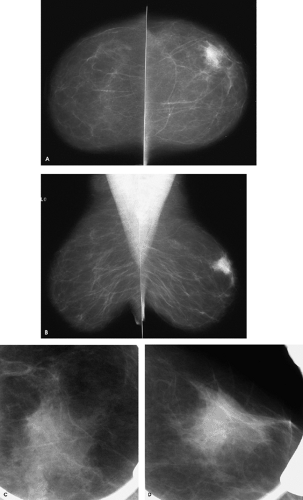 Figure 2.8. Initial screening study, 41-year-old woman. Craniocaudal (A) and mediolateral oblique (B) views. Craniocaudal (C) and mediolateral oblique (D) spot compression views. |
Patient 5
What do you think?
What BI-RADS® category would you assign, and what is your recommendation?
A focal area of parenchymal asymmetry is present in the upper outer quadrant of the left breast. It is of comparable size and density and is at the same approximate distance from the nipple on the two projections. Differential considerations include normal variant, hormone replacement therapy effect, asymmetry secondary to prior surgical excision of the corresponding tissue in the right breast, focal fibrosis, pseudoangiomatous stromal hyperplasia (PASH), posttraumatic changes (evolving hematoma, fat necrosis), mastitis, fibroadenolipoma (hamartoma), invasive ductal carcinoma not otherwise specified, invasive lobular carcinoma, and lymphoma.
If, as in this woman, no prior studies are available for comparison, spot compression views and possibly ultrasound with correlative physical examination can be undertaken to exclude an underlying malignancy.
BI-RADS® category 0: need additional imaging evaluation.
What do you think of this predominantly fatty pattern in a 41-year-old woman?
Although it is routinely suggested that mammography in young women is not very good because dense tissue precludes the detection of breast cancer, it is clear that age alone cannot be used to establish the density of the parenchymal pattern in an individual woman. Regardless of childbearing, young women can have completely fatty tissue and older, postmenopausal women can have dense tissue. It is also important to recognize that there is large intra- and interobserver variability in the application of arbitrarily defined parenchymal patterns. Additionally, the perceived density of a tissue pattern is dependent on technical factors. Some “extremely dense” tissue is inadequately exposed fibroglandular tissue.
What do you think now?
What BI-RADS® category would you assign at this point, and what is your recommendation?
Normal tissue is imaged on the spot compression views. The overall appearance and density of this tissue is different in the two projections; there is scalloping and fatty tissue is interspersed with the glandular tissue. There is a gradual change in density at the margins. In contrast, masses are three-dimensional with comparable size and density regardless of projection. They are also characterized by an abrupt change in density at the margins. The patient has no history of breast surgery and recalls no trauma to the left breast. Physical examination of this area is normal and symmetric with the comparable site on the contralateral breast. No tenderness is elicited. Ultrasound demonstrates normal tissue throughout the upper outer quadrant of the left breast. This is benign focal parenchymal asymmetry, a normal variant.
BI-RADS® category 2: benign finding. Annual screening mammography is recommended.
Patient 6
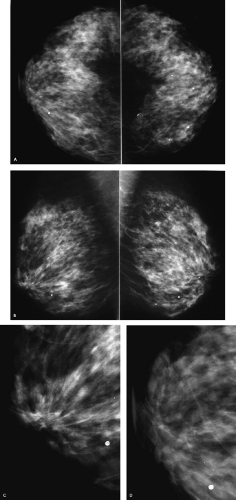 Figure 2.9. Screening study, 68-year-old woman. Craniocaudal (A) and mediolateral oblique (B) views. Mediolateral oblique (C) and craniocaudal (D) photographically coned views. Architectural distortion readily apparent on the mediolateral oblique view, more subtle on the craniocaudal view. |
How do you evaluate a screening mammogram?
The evaluation of screening mammograms can be approached in different ways. Develop a strategy that is systematic and use it consistently. Take a proactive approach, and actively send your eyes and brain looking for particular abnormalities in specific locations (subareolar area, medially on craniocaudal views, etc.). This helps you stay focused and minimizes the likelihood that you will miss significant findings. Whatever approach you settle on, it should include a review of the films for technical adequacy. Specifically, is the positioning acceptable? Has tissue and possibly a lesion been excluded (e.g., do you see tissue to the edge of any of the films)? Is glandular tissue adequately compressed and penetrated? Are the films high in contrast? Are there any artifacts that may preclude adequate interpretation of the films? Is there any blurring? Before focusing on perceiving localized findings, look for global or diffuse changes. These may be difficult to appreciate once you focus your attention on more subtle findings.
After evaluating the mammogram at a distance for technical adequacy and diffuse changes, look specifically (with and without a magnification lens) for masses, focal areas of asymmetry, architectural distortion, and calcifications. It is helpful to narrow your search, so on craniocaudal (CC) views, focus on the lateral, middle, and medial thirds of the breasts (Fig. 2.1). On the mediolateral oblique (MLO) views, focus on the upper, middle, and lower thirds of the breasts (Fig. 2.2). Search out potentially abnormal areas as you go back and forth between the right and the left breasts. Specifically, evaluate fat/glandular interfaces, the fatty stripe of tissue between pectoral muscle and glandular tissue on MLO views, the superior cone of tissue on the MLO views, subareolar areas, and the usually fatty tissue medially on CC views (Fig. 2.3). After developing a working hypothesis on a given mammogram, compare with prior studies and look at the history form for any pertinent information (family history of breast cancer or ovarian cancer, estrogen use, prior trauma or surgery, etc.).
What do you think?
In this patient, scattered dystrophic calcifications are present bilaterally. Did you find a potential abnormality? If you did not, look specifically for architectural distortion and move to the subareolar areas. Architectural distortion is present in the right subareolar area, best seen on the MLO view (Fig. 2.9C); it is not readily apparent on the CC view (Fig. 2.9D). Is it safe to assume that this is cancer? No! Benign-appearing lesions can turn out to be cancer, malignant-appearing lesions can reflect benign changes. Make no assumptions, or you will pigeonhole yourself and limit your ability to think through the possibilities. Most findings in the breast have benign and malignant etiologies in the differential. Our job is to sort through the possibilities accurately and efficiently.
What is your differential for architectural distortion?
Among the benign possibilities, consider fat necrosis related to trauma or prior surgery, mastitis, complex sclerosing lesions (sclerosing adenosis), papilloma, and focal fibrosis (rare). Invasive ductal carcinoma not otherwise specified (NOS), tubular carcinoma, ductal carcinoma in situ (rare), and invasive lobular carcinoma are among the invasive lesions that may present with architectural distortion. Armed with differential considerations, you can sort through them by integrating the imaging features of the lesion in question with the patient’s age, pertinent history, and physical examination. If you develop and routinely follow a simple, logical, and systematic approach, the next appropriate step becomes readily apparent and is justifiable. This approach is rarely misleading.
What, if any, history would keep you from calling this patient back?
What BI-RADS® assessment category would you assign, and what is your recommendation?
In this patient, the overall characteristics of the lesion include long spicules, no significant central density, and a more pronounced appearance in one of the two routine views. It is critical to establish if the patient has had a biopsy (or significant trauma) in the right subareolar area. If there is a history of prior surgery, the location of the surgical procedure has to correspond directly to the area of distortion. Don’t hesitate to examine the patient to establish the presence of a subtle periareolar scar even when the patient does not recall a prior breast biopsy. A complex sclerosing lesion is a good possibility in a woman with this type of lesion and no history of surgery or apparent scar on physical examination. Complex sclerosing lesions are often seen better in one projection and, given their size, usually have no corresponding palpable abnormality on physical examination. In considering mastitis, the breast is usually tender; there may be associated erythema and warmth as well as a history of prior inflammatory changes in the subareolar area.
In thinking about the malignant possibilities, an invasive ductal carcinoma (NOS) of this size and in this location will almost certainly have physical findings, including a palpable abnormality, dimpling, and possibly nipple retraction. Tubular carcinomas are usually fairly small and are more commonly identified in younger women (in their 40s). Invasive lobular carcinomas are more common in older patients, and physical findings are often subtle.
This patient has had surgery in the right subareolar area corresponding to the site of distortion. The findings reflect fat necrosis related to the prior biopsy. Architectural distortion related to prior surgery is often planar and therefore better seen in one projection, as in this patient. No additional evaluation is indicated.
BI-RADS® category 2: benign finding. Annual screening mammography is recommended.
Patient 7
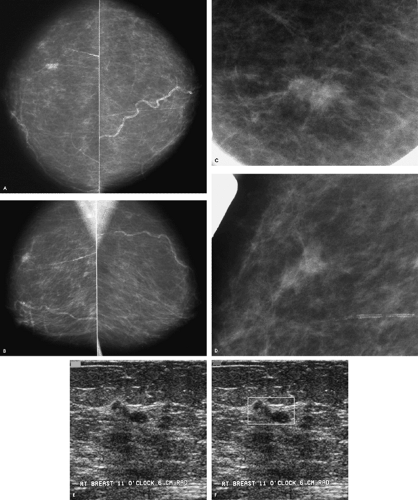 Figure 2.10. Screening study, 68-year-old woman. Craniocaudal (A) and mediolateral oblique (B) views. Craniocaudal (C) and mediolateral oblique (D) spot compression views, right breast. Ultrasound image (E), radial (RAD) projection of the lesion. Ultrasound image (F), radial (RAD) projection. The lesion is contained in the box. |
What do you think?
What BI-RADS® assessment category would you assign, and what is your recommendation?
There are arterial calcifications bilaterally. Did you notice a mass in the right breast? This is new compared with prior studies (not shown). Additional evaluation is recommended. BI-RADS® category 0: need additional imaging evaluation.
Do you have any additional observations?
Technically, are you happy with this study?
Be specific in describing the problem
Positioning on this study is not optimal. There is insufficient pectoral muscle on the mediolateral oblique (MLO) views. Ideally, pectoral muscle should be seen to the level of the nipple; it should be thick in the axilla and have a convex anterior margin. Given the triangular shape of the muscle in this patient, several things went wrong during positioning. It is likely that an incorrect angle of obliquity was selected, the muscles were not relaxed, and the breasts were not adequately mobilized medially (or if they were, the patient pulled out during positioning).
On the craniocaudal (CC) views, a significant amount of posterior tissue is excluded from the images. In determining if an adequate amount of tissue has been included on the CC views, look for pectoral muscle posteriorly or for cleavage medially. If neither of these is seen, measure the posterior nipple line (PNL) on the MLO views (and remember that in this patient, positioning on the MLO views is not optimal, so the PNL measurement is not an optimal measure of the amount of tissue this patient has) and compare it to that measured on the CC views (Fig. 2.4E, F). The PNL measurement on the CC view should be within 1 cm of that measured on the MLO view. It is not in this patient. Additionally, if you look at the length of the calcified artery laterally on the right CC and the relationship of the lesion to the edge of the film between CC and MLO views, it is clear that posterior tissue has been excluded on the CC views.
What do you think?
How would you describe the finding, and at what clock position would you expect to find this lesion?
The spot compression views confirm the presence of a 1-cm irregular mass with spiculated margins. A biopsy is indicated based on the mammographic findings.
An irregular, hypoechoic mass with angular margins is imaged at the 11 o’clock position, 6 cm from the right nipple, corresponding to the expected location of the lesion seen mammographically.
BI-RADS® category 4: suspicious abnormality, biopsy should be considered. An ultrasound-guided core biopsy is done at the time of the diagnostic evaluation.
A poorly differentiated, invasive ductal carcinoma is reported histologically following the ultrasound guided core biopsy. A 1.2-cm, grade III, invasive ductal carcinoma is reported on the lumpectomy specimen. No metastatic disease is identified in four excised sentinel lymph nodes; [pT1c, pN0(sn)(i—), pMX; Stage I].
Patient 8
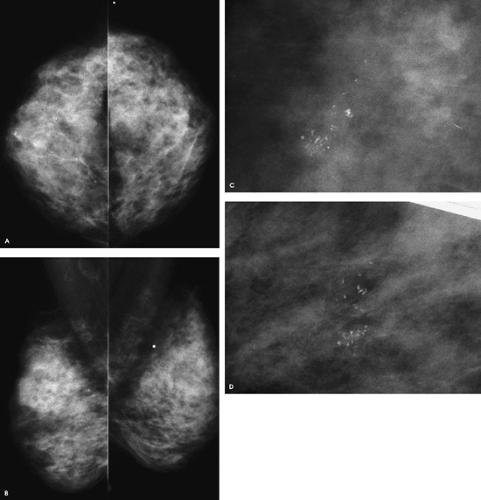 Figure 2.11. Screening study, 51-year-old woman. Craniocaudal (A) and mediolateral oblique (B) views. The metallic BB on the left is on a skin lesion. No history of breast surgery or significant trauma. Craniocaudal (C) and mediolateral oblique (D), double spot compression magnification views. |
Any observations?
What BI-RADS® assessment category would you assign, and what is your recommendation?
Systematically review the images and actively look for potential lesions. In addition to splitting the craniocaudal (CC) and mediolateral oblique (MLO) views into thirds and evaluating the locations where cancers are likely to develop, look specifically for diffuse changes, masses, distortion, asymmetry, and calcifications. If you focus down with a magnification lens and look specifically for calcifications on every screening mammogram you review, you are unlikely to miss the relevant finding in this patient. Did you see the cluster of calcifications anteriorly at approximately the 6 o’clock position in the right breast? With what degree of confidence can you characterize these, and how definitive can you be with respect to their significance? Why not get more information in the form of double spot compression magnification views? There are other calcifications posteriorly (close to the edge of the film medially) in the lower inner quadrant on the right, but these contain lucent centers and are benign.
BI-RADS® category 0: need additional imaging evaluation.
What do you think?
What BI-RADS® assessment category would you assign, and what is your recommendation?
On the double spot compression magnification views, the morphology of the calcifications is much better demonstrated, as is the extent of the lesion. The calcifications in this cluster are pleomorphic, and there are linear forms. Armed with high-quality magnification views, our confidence in the likely diagnosis of ductal carcinoma in situ is increased significantly, and the need for a biopsy is easily justified.
BI-RADS® category 4: Suspicious abnormality; biopsy should be considered. A stereotactically guided needle biopsy is done on the same day as the magnification views. A high-nuclear-grade ductal carcinoma in situ with central necrosis is diagnosed on the core biopsy. A 1-cm area of high-nuclear-grade ductal carcinoma in situ with central necrosis and no associated invasion is described histologically on the lumpectomy specimen. No sentinel lymph node biopsy is done [pTis(DCIS), pNX, pMX; Stage 0].
Patient 9
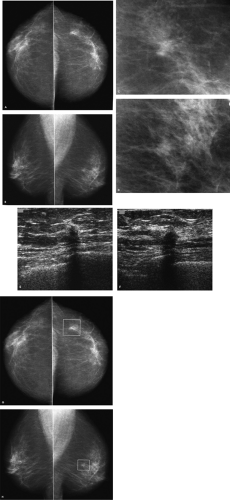 Figure 2.12. Screening study, 73-year-old woman. Craniocaudal (A) and mediolateral oblique (B) views, left breast. No prior films available for comparison. Craniocaudal (C) and mediolateral oblique (D) spot compression views, left breast. Ultrasound images in radial (RAD) (E) and antiradial (ARAD) (F) projections, left breast. Craniocaudal (G) and mediolateral oblique (H) views. Box indicating location of potential mammographic abnormality. |
Would you agree with a BI-RADS® assessment category 2: benign finding?
There is a mass in the left breast at approximately the 3 o’clock position, 4 cm from the left nipple. Did you see it (Fig. 2.12G, H)? What did you think? Good for you, if you are not willing to accept this as an intramammary lymph node. Although it may be that a fatty hilum and well-circumscribed margins are demonstrated with spot compression views, on these screening views no fatty hilum is apparent and the margins are not well defined. Remember: Make no assumptions. With what degree of certainty can you say this is a lymph node? If you are not sure, call the patient back for additional evaluation.
BI-RADS® category 0: need additional imaging evaluation.
What do you think now?
A 1-cm spiculated mass is confirmed on the spot compression views. A biopsy is indicated. An ultrasound is done to determine whether the lesion is identified on ultrasound; if it is, ultrasound guidance can be used for the core biopsy.
How would you describe the ultrasound findings?
A vertically oriented, irregular hypoechoic mass with indistinct and angular margins, shadowing, and associated distortion of the surrounding tissue is imaged at the 3 o’clock position, 4 cm from the left nipple, correlating to the expected location of the lesion seen mammographically. With the additional views and the ultrasound we can issue a succinct, definitive report on the finding, the likely significance, and our recommendations. Would you now agree with the assignment of BI-RADS® category 4: suspicious abnormality; biopsy should be considered.
An invasive ductal carcinoma is diagnosed following an ultrasound-guided core biopsy. A 0.7-cm invasive ductal carcinoma with tubular features (grade I) is diagnosed on the lumpectomy specimen. No metastatic disease is diagnosed in two excised sentinel lymph nodes [pT1b, pN0(sn)(i—), pMX; Stage I].
Patient 10
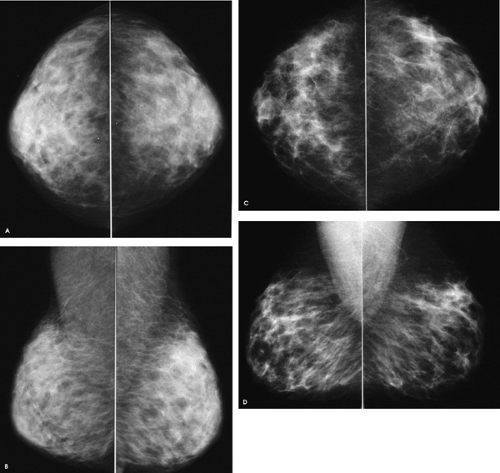 Figure 2.13. Screening study, 38-year-old woman. Craniocaudal (A) and mediolateral oblique (B) views. Comparison study, craniocaudal (C) and mediolateral oblique (D) views. |
| RCC | RCC | LCC | LCC | RMLO | RMLO | LMLO | LMLO | |
|---|---|---|---|---|---|---|---|---|
| Factor | (A) | (C) | (A) | (C) | (B) | (D) | (B) | (D) |
| kV | 26 | 26 | 26 | 26 | 26 | 27 | 26 | 27 |
| mAs | 36 | 294 | 41 | 334 | 47 | 363 | 43 | 352 |
| Comp(mm) | 22 | 67 | 24 | 71 | 24 | 74 | 24 | 72 |
| Target/filter | mo/mo | mo/rh | mo/mo | mo/rh | mo/mo | mo/rh | mo/mo | mo/rh |
What do you think?
Are these mammograms from two different women?
If they are from the same woman, what is your working hypothesis?
Are there any significant findings in either mammogram?
These mammograms are normal and from the same woman, taken 20 months apart. In the interval, she lost 150 pounds. On the current study (Fig. 2.13A, B), breast size is decreased and parenchymal density is increased, with a concomitant decrease in fat compared with the study from 20 months before (Fig. 2.13C, D). The changes are bilateral and symmetric. There is no skin or trabecular thickening. The breasts are significantly thinner, as evidenced by the millimeters of compression used for exposure on the current study compared with 20 months before. Given similar kilovoltage peaks on both studies, the resulting milliamperage output is consistently lower on the current images. Also, note that rhodium kicked in for all of the films done on the comparison study.
Given the milliamperage output on the current study, what could the technologist have done to improve image quality?
Image contrast is partially related to the voltage used for exposure. As you increase voltage, you decrease image contrast. Optimally, you want to use a high enough voltage to penetrate the tissue adequately, but not much more than that. At a given voltage, the resulting amperage also needs to be considered, because this indirectly reflects the length of the exposure. As the amperage is increased, exposure time is increased, and as exposure time increases, motion blur may become an issue if the patient is unable to hold her breath. If, at a given voltage, the resulting amperage is high (>400 mAs) and the tissue is not adequately exposed, either voltage or compression (or both) need to be increased. As voltage is increased, the resulting amperage (and exposure time) decreases; as voltage is decreased, the resulting amperage (and exposure time) increases. In this woman, the resulting amperages on the current study are well below 400 mAs, so the voltage can be lowered without sacrificing adequate exposure of the tissue. As voltage is lowered, contrast is increased, improving overall image quality. Did you notice the low image contrast on the current images? Overall, the images (and particularly the fat) look gray, reflecting the poor contrast.
What is your differential for diffuse breast changes?
Differential considerations for diffuse changes that are usually unilateral, although rarely can be bilateral, include radiation therapy effect, inflammatory changes (e.g., mastitis), trauma, ipsilateral axillary adenopathy with lymphatic obstruction, dialysis shunt in the ipsilateral arm with fluid overload, invasive ductal carcinoma not otherwise specified, inflammatory carcinoma, invasive lobular carcinoma, or lymphoma. Invasive lobular carcinoma can lead to increases in breast density and size, or a decrease in breast size (the shrinking breast). Differential considerations for diffuse changes that are usually bilateral, although they can be unilateral, include hormone replacement therapy (e.g., estrogen), weight changes, congestive heart failure, renal failure with fluid overload, and superior vena cava syndrome. Additional rare benign causes include granulomatous mastitis, coumadin necrosis, arteritis, and autoimmune disorders (e.g., scleroderma). Obtaining a thorough history, examining the patient, and obtaining an ultrasound are often helpful in sorting through the differential considerations.
BI-RADS® category 1: negative. Next screening mammogram is recommended at age 40.
Patient 11
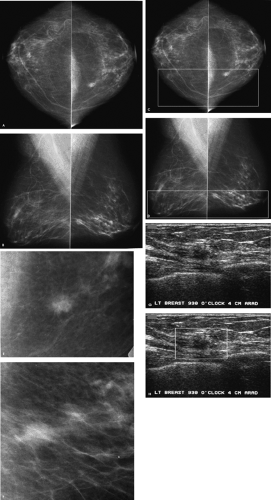 Figure 2.14. Screening study, 74-year-old woman. Craniocaudal (A) and mediolateral oblique (B) views. Craniocaudal (C) and mediolateral oblique (D) views with boxes on the medial and lower thirds of the breasts, respectively. Craniocaudal (E) and mediolateral oblique (F) spot compression views, left breast. Ultrasound image (G), antiradial (ARAD) projection, left breast. Ultrasound image (H), antiradial (ARAD) projection, left breast at the 9:30 o’clock position, 4 cm from the left nipple. A box delineates the mass. |
What do you think?
Is this a normal mammogram, or do you think additional evaluation is indicated?
In this patient, by splitting the images (Fig. 2.14C, D) in thirds and focusing your attention to the medial portions of the breasts on the craniocaudal (CC) views, a mass is detected medially in the left breast. On the mediolateral oblique (MLO) views, the corresponding mass is imaged in tissue projecting on the lower third of the left breast. If they are available, previous films will be helpful in assessing a change and should be requested before calling the patient back for a diagnostic evaluation. In the absence of comparison films, or if this represents a change when comparison is made to several sequential mammograms, additional evaluation is indicated.
BI-RADS® category 0: need additional imaging evaluation.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


