Shoulder Procedures
KEY FACTS
Preprocedure
 Glenohumeral joint aspiration (suspected infection) or injection (contrast for arthrography; adhesive capsulitis symptom relief)
Glenohumeral joint aspiration (suspected infection) or injection (contrast for arthrography; adhesive capsulitis symptom relief)
 Subacromial-subdeltoid (SA-SD) bursal injection (symptom relief) or aspiration (suspected infection)
Subacromial-subdeltoid (SA-SD) bursal injection (symptom relief) or aspiration (suspected infection)
 Calcific tendinitis (symptom relief)
Calcific tendinitis (symptom relief)
 Rotator cuff tendinosis or tear (symptom relief and to promote healing)
Rotator cuff tendinosis or tear (symptom relief and to promote healing)
 Acromioclavicular joint injection (symptomatic relief)
Acromioclavicular joint injection (symptomatic relief)

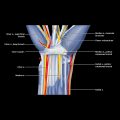
Clinical photo of a patient with shoulder dislocation shows needle (22-g spinal)  position for lateral long-axis approach to posterior glenohumeral joint for contrast injection before MR arthrography.
position for lateral long-axis approach to posterior glenohumeral joint for contrast injection before MR arthrography.

Subsequent axial MR arthrogram T1 FS (same patient) shows glenohumeral joint distension. Note anterior capsular stripping  and labral avulsion
and labral avulsion  . US-guided MR arthrography is a commonly performed procedure.
. US-guided MR arthrography is a commonly performed procedure.

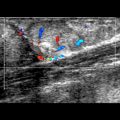
Longitudinal US shows moderate-severity calcific tendinitis of the supraspinatus tendon  . The largest calcification
. The largest calcification  , calcification with the most focal edema, or calcification that most closely correlates with symptoms are best targeted for percutaneous lavage and aspiration.
, calcification with the most focal edema, or calcification that most closely correlates with symptoms are best targeted for percutaneous lavage and aspiration.

Longitudinal US shows aspiration of calcific content  using an 18-g needle, connected to a syringe containing a saline-lignocaine mixture. Lavage and aspiration are performed in series.
using an 18-g needle, connected to a syringe containing a saline-lignocaine mixture. Lavage and aspiration are performed in series.
PREPROCEDURE
Indications
PROCEDURE
Procedure Steps
 General practical points irrespective of anterior (rotator cuff interval) or posterior approach
General practical points irrespective of anterior (rotator cuff interval) or posterior approach
 Posterior approach
Posterior approach
 Rotator interval approach
Rotator interval approach
 10-20 mL of contrast solution is injected until joint capsule is satisfactorily distended
10-20 mL of contrast solution is injected until joint capsule is satisfactorily distended
 Volume of injection is determined according to patient’s comfort level and resistance to injection
Volume of injection is determined according to patient’s comfort level and resistance to injection
 Patients with severe adhesive capsulitis will feel distension after only small volume (5-10 mL) of fluid injected into joint
Patients with severe adhesive capsulitis will feel distension after only small volume (5-10 mL) of fluid injected into joint
 Patients following shoulder dislocation can accommodate larger volumes (15-20 mL)
Patients following shoulder dislocation can accommodate larger volumes (15-20 mL) ![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Shoulder Procedures