Shoulder Ultrasound
KEY FACTS
GENERAL CONSIDERATIONS

Clinical photograph shows Crass position during examination of supraspinatus tendon on long-axis view. Back of the hand is placed across the back, which internally rotates the shoulder, bringing the tendon out from underneath the acromion.

Clinical photograph shows the modified Crass position. The hand is placed on the ipsilateral back pocket, producing less internal rotation than the Crass position. The anterior edge of supraspinatus can be more clearly seen, especially on short-axis views.

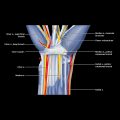
Longitudinal US along the supraspinatus tendon shows anterior fibers inserting into the anterior facet  of the greater tuberosity. Focal anisotropy
of the greater tuberosity. Focal anisotropy  due to fiber orientation is present. This is a common site for anisotropy.
due to fiber orientation is present. This is a common site for anisotropy.

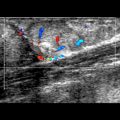
Longitudinal US of the supraspinatus tendon in the same location shows alteration in the tendon fiber orientation with lessening of anisotropic effect  . Insonation angle can be changed by angling the transducer or altering the patient’s position.
. Insonation angle can be changed by angling the transducer or altering the patient’s position.
GENERAL CONSIDERATIONS
Clinical Indications for Shoulder US
TECHNIQUE
Full Standardized Examination
Patient Position and Approach
Long Head of Biceps Tendon
 Align transducer transversely across bicipital groove
Align transducer transversely across bicipital groove
 Scan proximally to uppermost aspect of bicipital groove and distally to where pectoralis major tendon passes over biceps tendon
Scan proximally to uppermost aspect of bicipital groove and distally to where pectoralis major tendon passes over biceps tendon
 Most biceps pathology is localized to proximal-most segment known as “genu” of long head of biceps tendon
Most biceps pathology is localized to proximal-most segment known as “genu” of long head of biceps tendon
 Slightly extending arm will allow one to see more of proximal biceps tendon
Slightly extending arm will allow one to see more of proximal biceps tendon
 ± internally/externally rotate arm to test for biceps subluxation
± internally/externally rotate arm to test for biceps subluxation
 Rotate transducer 90° to align longitudinal to biceps tendon, focusing particularly on proximal end of tendon
Rotate transducer 90° to align longitudinal to biceps tendon, focusing particularly on proximal end of tendon
Rotator Interval
 Scan transversely across biceps tendon at and proximal to uppermost portion of bicipital groove
Scan transversely across biceps tendon at and proximal to uppermost portion of bicipital groove
 Proximal, mid-, and distal portions of rotator interval should be examined
Proximal, mid-, and distal portions of rotator interval should be examined
 Uppermost part of bicipital groove equates to distal end of rotator interval
Uppermost part of bicipital groove equates to distal end of rotator interval
 Coracohumeral ligament (CHL) seen as echogenic band, ~ 1.5 mm thick, superficial to biceps tendon
Coracohumeral ligament (CHL) seen as echogenic band, ~ 1.5 mm thick, superficial to biceps tendon
 CHL joins with superior glenohumeral ligament medially forming bicipital sling
CHL joins with superior glenohumeral ligament medially forming bicipital sling
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree