Sinonasal Squamous Cell Carcinoma
Michelle A. Michel, MD
Key Facts
Terminology
Malignant epithelial tumor with squamous cell or epidermoid differentiation
Imaging
Location: Maxillary antrum involved > 80%
CT findings
Soft tissue density mass with irregular margins
Aggressive bone destruction
MR findings
↓ T2 signal due to ↑ N:C ratio
Enhances to lesser degree than other sinonasal malignancies
Multiplanar enhanced MR optimal for tumor mapping, detection of PNTS & nodes
Top Differential Diagnoses
Sinonasal adenocarcinoma
Sinonasal undifferentiated carcinoma (SNUC)
Invasive fungal sinusitis
Sinonasal non-Hodgkin lymphoma
Wegener granulomatosis
Pathology
Risk factors: Inhaled wood dust, metallic particles, chemicals, HPV, inverted papilloma
Formaldehyde & asbestos exposure may ↑ risk
Human papilloma virus, pre- or coexisting inverted papilloma ↑ risk
Clinical Issues
Symptoms mimic chronic sinusitis & delay diagnosis
Age at presentation: 50-70 years old
Most common malignancy of sinonasal area
15% maxillary sinus SCCa have malignant adenopathy
Overall 5-year survival: 60%
Combined surgery & XRT most common treatment
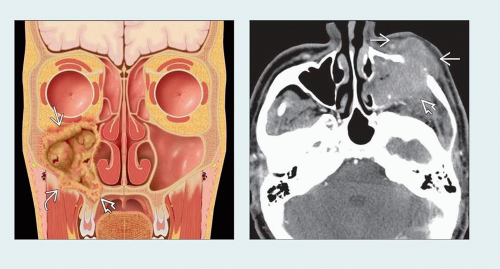 (Left) Coronal graphic shows the typical features of an aggressive right maxillary SCCa with destruction of the maxillary sinus walls. Extension into the orbit  , maxillary alveolus , maxillary alveolus  , and buccal space , and buccal space  is noted. (Right) Axial CECT shows the typical location and appearance of an antral SCCa. There is extension into the premaxillary soft tissues anteriorly is noted. (Right) Axial CECT shows the typical location and appearance of an antral SCCa. There is extension into the premaxillary soft tissues anteriorly  and through the posterior maxillary wall into the infratemporal fossa and through the posterior maxillary wall into the infratemporal fossa  . . |
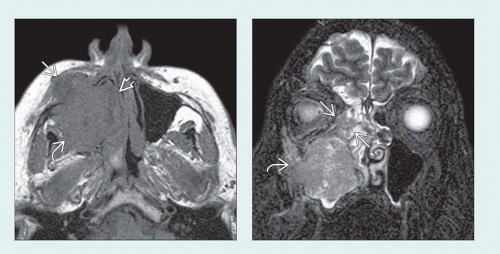 (Left) Axial T1WI MR shows a large antral SCCa. The signal of the mass is similar to other soft tissues. There is extension anteriorly into the premaxillary soft tissues  , medially into the nasal cavity , medially into the nasal cavity  , and posteriorly into the masticator space , and posteriorly into the masticator space  . (Right) Coronal T2WI FS MR in the same patient demonstrates ethmoid sinus involvement . (Right) Coronal T2WI FS MR in the same patient demonstrates ethmoid sinus involvement  and masticator space extension and masticator space extension  . The low T2 signal of this mass is consistent with high cellularity and N:C ratio. . The low T2 signal of this mass is consistent with high cellularity and N:C ratio. |
TERMINOLOGY
Abbreviations
Squamous cell carcinoma (SCCa)
Synonyms
Epidermoid carcinoma, transitional carcinoma, nonkeratinizing carcinoma, respiratory mucosal carcinoma
Definitions
Malignant epithelial tumor growing from sinus surface epithelium into sinus lumen with squamous cell or epidermoid differentiation
IMAGING
General Features
Best diagnostic clue
Aggressive antral soft tissue mass with invasion & destruction of sinus walls
Location
75% arise in sinuses; 30% arise primarily in nose
Maxillary antrum (85%), ethmoid (10%), frontal/sphenoid (< 5%)
Radiologist creates presurgical tumor map of spread
Medial: Nasal cavity → ethmoid sinuses
Anterior: Subcutaneous tissues of cheek
Posterior: Retroantral fat pad, pterygopalatine fossa (PPF) & masticator space
Lateral: Malar eminence & subcutaneous tissues
Superior: Through orbital floor into orbit proper or via PPF → inferior orbital fissure → orbit
Perineural tumor spread (PNTS): Inferior orbital nerve or PPF → V2 (foramen rotundum) → cavernous sinus
Size
Usually fills maxillary antrum
Morphology
Well defined to poorly defined with irregular, spiculated margins
CT Findings
CECT
Solid, moderately enhancing mass with aggressive bone destructionRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


