SONOGRAM ABBREVIATIONS
Ao Aorta
Azv Azygous vein (ascending lumbar vein)
Ca Celiac artery
CBD Common bile duct
CHa Common hepatic artery
CHD Common hepatic duct
CIa Common iliac artery
Cr Crus of the diaphragm
Du Duodenum
GBl Gallbladder
Gda Gastroduodenal artery
Hea Hepatic artery
Hev Hepatic vein
IMa Inferior mesenteric artery
IMv Inferior mesenteric vein
IVC Inferior vena cava
K Kidney
L Liver
LGa Left gastric artery
LGv Left gastric vein
LHev Left hepatic vein
LPv Left portal vein
LRa Left renal artery
LRv Left renal vein
MHev Middle hepatic vein
P Pancreas
PHa Proper hepatic artery
Ps Psoas muscles
Pv Portal vein
QL Quadratus lumborum
RA Rectus abdominis
RGv Right gastric vein
RHev Right hepatic vein
RPv Right portal vein
RRa Right renal artery
RRv Right renal vein
S Spine
SGv Splenogastric vein
SMA Superior mesenteric artery
SMV Superior mesenteric vein
Spa Splenic artery
Spv Splenic vein
St Stomach
Because the bony landmarks visible with other imaging modalities are not available and gas may limit the ultrasound field of view, recognizing normal anatomic landmarks is crucial for proper orientation. Vascular structures are the most important in defining location, but normal muscular structure and organ position must also be known.
Figure 6-1. ![]() Commonly visualized vessels arising from the aorta are the celiac artery, splenic artery, left gastric artery, common hepatic artery, proper hepatic artery, gastroduodenal artery, right and left renal arteries, superior mesenteric artery, inferior mesenteric artery, and—below the aortic bifurcation at the level of the fourth lumbar vertebra—the right and left common iliac arteries. Only the portion of the aorta below the diaphragm is visualized on an abdominal study.
Commonly visualized vessels arising from the aorta are the celiac artery, splenic artery, left gastric artery, common hepatic artery, proper hepatic artery, gastroduodenal artery, right and left renal arteries, superior mesenteric artery, inferior mesenteric artery, and—below the aortic bifurcation at the level of the fourth lumbar vertebra—the right and left common iliac arteries. Only the portion of the aorta below the diaphragm is visualized on an abdominal study.
SONOGRAM ABBREVIATIONS
KEY ANATOMICAL STRUCTURES
ARTERIES
Aorta (Abdominal). Main trunk of the arterial system (see Figs. 6-1 and 6-5). Lies anterior to the spine and bifurcates into the right and left common iliac arteries at the level of the umbilicus.
Celiac Artery (Axis, Trunk). Arises just below the liver from the anterior aorta and is usually only 2 to 3 cm in length (see Figs. 6-1, 6-2, and 6-5). It almost immediately divides into the splenic artery, left gastric artery, and common hepatic artery.
Common Femoral Arteries. Seen in the inguinal region, the common femoral arteries arise from the iliac arteries and extend into the upper thigh (see Fig. 50-1). A branch—the profunda femoris—originates just below the inguinal ligament.
Common Iliac Arteries. Originate from the aorta at the level of the umbilicus and extend toward the groin (Fig. 6-1). Less than 15 mm in diameter at their origin is normal.
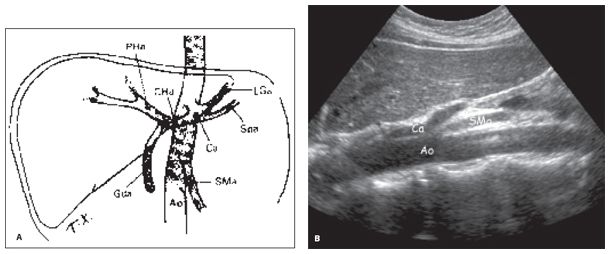
Figure 6-2. ![]() A. The vessel arising from the aorta, closest to the diaphragm is the celiac artery. This vessel is a 1- to 2-cm trunk that bifurcates into the splenic and common hepatic arteries. The common hepatic artery then bifurcates into the proper hepatic artery and gastroduodenal artery. The superior mesenteric artery (SMA) arises from the anterior surface of the aorta at a level just inferior to the celiac artery. The less-frequently visualized left gastric artery originates from the celiac artery. B. Longitudinal ultrasound of the aorta showing the celiac artery arising anteriorly, with the SMA arising below it.
A. The vessel arising from the aorta, closest to the diaphragm is the celiac artery. This vessel is a 1- to 2-cm trunk that bifurcates into the splenic and common hepatic arteries. The common hepatic artery then bifurcates into the proper hepatic artery and gastroduodenal artery. The superior mesenteric artery (SMA) arises from the anterior surface of the aorta at a level just inferior to the celiac artery. The less-frequently visualized left gastric artery originates from the celiac artery. B. Longitudinal ultrasound of the aorta showing the celiac artery arising anteriorly, with the SMA arising below it.
Gastroduodenal Artery. Originates from the common hepatic trunk and supplies the stomach and duodenum (Figs. 6-1, 6-2, and 6-3). It is a landmark delineating the anterolateral aspect of the head of the pancreas.
Hepatic Artery (Common). Originates from the celiac trunk and courses toward the liver. It branches into the proper hepatic artery and the gastroduodenal artery (Figs. 6-1 and 6-2). Supplies the stomach, pancreas, duodenum, liver, gallbladder, and greater omentum.
Hepatic Artery (Proper). A branch of the common hepatic artery that supplies the liver and gallbladder (Figs. 6-1 and 6-2). It runs medial to the common bile duct and anterior to the portal vein into the liver within the porta hepatis.
Inferior Mesenteric Artery. Originates from the abdominal aorta close to the umbilicus (Fig. 6-1). Supplies the left portion of the transverse colon, the descending and sigmoid colon, and part of the rectum. It is not usually visualized by ultrasound except at its origin.
Left Gastric Artery. Arises from the superior margin of the celiac axis and can be seen by ultrasound for only 1 or 2 cm (Figs. 6-1 and 6-2); supplies the stomach.
Renal Arteries, Right and Left. Originate from the abdominal aorta just below the level of the SMA. They supply the kidneys, adrenals, as well as the ureters, and are often best seen when the patient is in the appropriate decubitus position. The left renal artery arises from the posterolateral wall of the aorta and enters the left renal hilum. The right arises from the posterolateral wall of the aorta, runs posterior to the inferior vena cava (IVC), and enters the right renal hilum (Fig. 6-1).
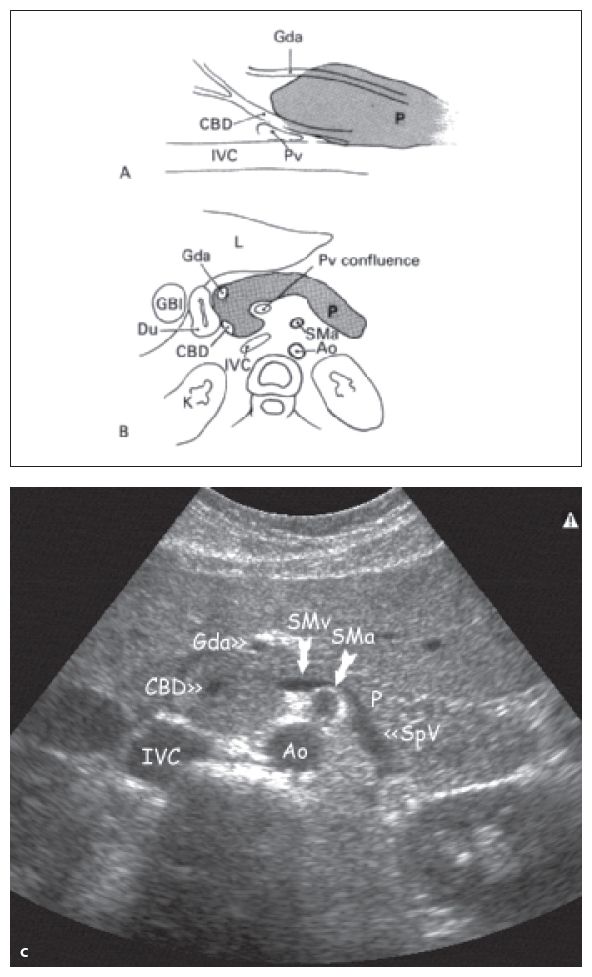
Figure 6-3. ![]() The gastroduodenal artery outlines the anterolateral margin of the head of the pancreas, whereas the common bile duct marks the posterolateral margin. A. Longitudinal diagram. B. Transverse diagram. C. Transverse ultrasound image.
The gastroduodenal artery outlines the anterolateral margin of the head of the pancreas, whereas the common bile duct marks the posterolateral margin. A. Longitudinal diagram. B. Transverse diagram. C. Transverse ultrasound image.
Replaced Right Hepatic Artery. A normal variant in which the right hepatic artery arises from the SMA, rather than the proper hepatic artery and celiac axis. (Fig. 6-4).
Splenic Artery. Originates from the celiac trunk (Fig. 6-1, 6-2, and 6-5) and courses superior to the body and tail of the pancreas. It primarily supplies the spleen.
Superior Mesenteric Artery. Originates from the anterior abdominal aorta, just below the celiac axis and runs parallel to the aorta (Figs. 6-1, 6-4, and 6-5). It lies posterior to the body of the pancreas. Supplies the small bowel, cecum, ascending colon, and part of the transverse colon.
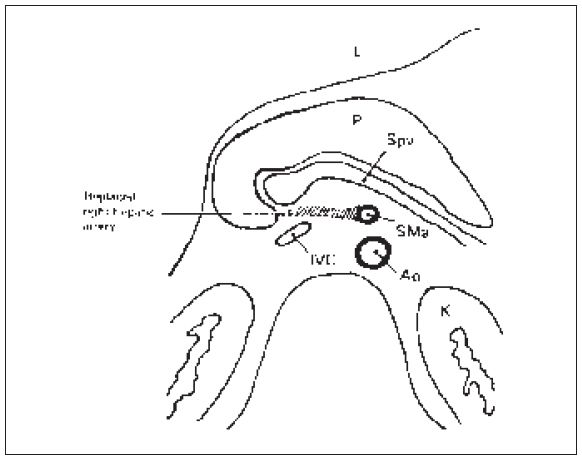
Figure 6-4. ![]() At the level of the splenic vein and pancreas, a normal variant can sometimes be visualized. The replaced right hepatic artery originates from the superior mesenteric artery to supply the liver.
At the level of the splenic vein and pancreas, a normal variant can sometimes be visualized. The replaced right hepatic artery originates from the superior mesenteric artery to supply the liver.
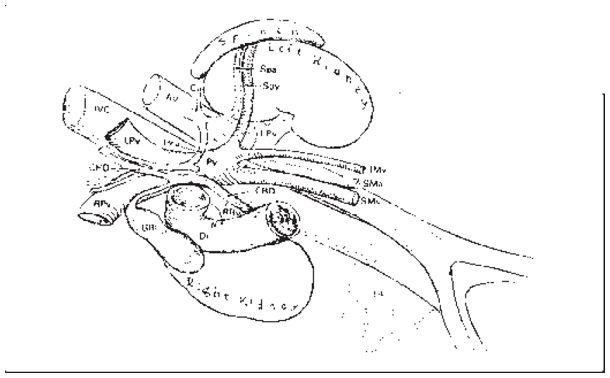
Figure 6-5. ![]() Oblique view, showing the relationship of the portal vein, IVC, and aorta to the kidneys and gallbladder. The major branches of the portal vein, hepatic artery, and common hepatic duct in relationship to the porta hepatis are shown.
Oblique view, showing the relationship of the portal vein, IVC, and aorta to the kidneys and gallbladder. The major branches of the portal vein, hepatic artery, and common hepatic duct in relationship to the porta hepatis are shown.
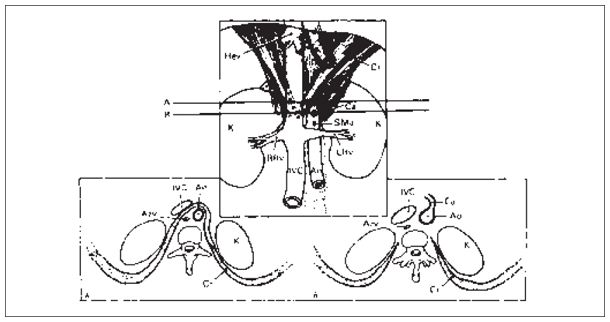
Figure 6-6. ![]() The crus of the diaphragm can be visualized anterior to the aorta above the level of the celiac artery. Below that level, it extends along the lateral aspects of the vertebral column only. A. A transverse section at a higher level shows the crus posterior to the IVC and anterior to the aorta. The infrequently visualized azygos vein is seen posterior to the crus. B. At a lower level, transversely, the crus is seen only at the lateral vertebral margins extending posteriorly.
The crus of the diaphragm can be visualized anterior to the aorta above the level of the celiac artery. Below that level, it extends along the lateral aspects of the vertebral column only. A. A transverse section at a higher level shows the crus posterior to the IVC and anterior to the aorta. The infrequently visualized azygos vein is seen posterior to the crus. B. At a lower level, transversely, the crus is seen only at the lateral vertebral margins extending posteriorly.
VEINS
Azygous Vein. Lies posterior to the IVC and is not usually seen unless enlarged secondary to congestive heart failure or portal hypertension (see Fig. 6-7).
Collaterals. Accessory vessels that develop when portal vein pressure is increased (e.g., portal hypertension) (Fig. 6-6). Collaterals can be seen in the region of the pancreas, around the esophagogastric junction (anterior to the upper portion of the aorta), in the porta hepatis, and in the splenic hilum (Fig. 6-7).
Confluence. The junction of the superior mesenteric vein and splenic vein, which forms the main portal vein (see Figs. 6-5 and 6-9).
Femoral Veins. Lie medial to the femoral arteries in the groin and upper thigh. They are normally larger than the arteries. These veins normally compress easily and do not pulsate (see Figs. 50-2 and 50-3).
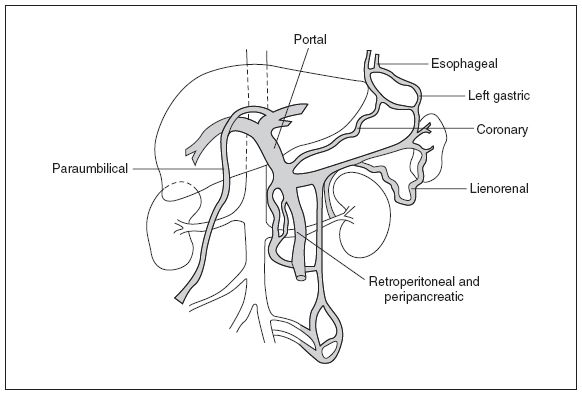
Figure 6-7. ![]() Diagram showing some of the collateral routes established when portal hypertension exists. The paraesophageal, left gastric, coronary, paraumbilical, lienorenal, retroperitoneal, and peripancreatic collaterals are demonstrated.
Diagram showing some of the collateral routes established when portal hypertension exists. The paraesophageal, left gastric, coronary, paraumbilical, lienorenal, retroperitoneal, and peripancreatic collaterals are demonstrated.
Hepatic Veins. Drain the liver and empty into the IVC just below the diaphragm (see Figs. 6-8, 6-9, and 6-14). The right hepatic vein divides the liver into right anterior and right posterior segments. The left hepatic vein divides the left medial and left lateral segments of the liver. The middle hepatic vein divides the right and left lobes of the liver. (See Chapter 8 for a discussion of hepatic anatomy and the Couinaud-Bismuth system for describing parts of the liver.)
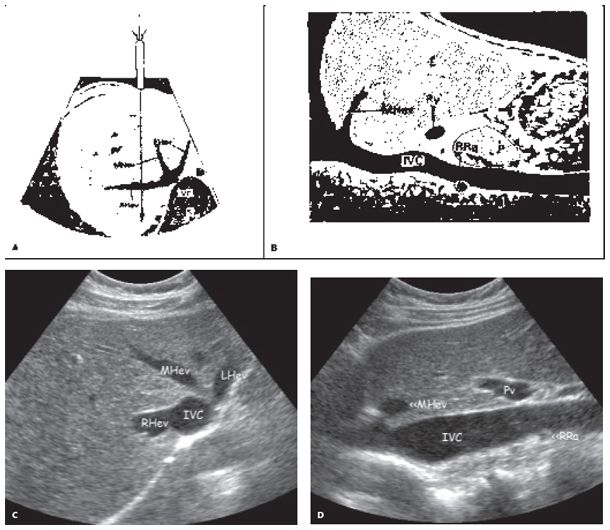
Figure 6-8. ![]() Hepatic veins. A. Transverse diagram, using a slightly cephalad angulation. The left, middle, and right hepatic veins can be imaged as they empty into the IVC just beneath the right diaphragm. B. Longitudinal diagram. The middle hepatic vein is shown as it empties into the IVC at the level of the right diaphragm. The main branch of the portal vein is seen in its extrahepatic location just superior to the head of the pancreas. The right renal artery is visualized posterior to the IVC. (C) Transverse ultrasound image corresponding to (A). (D) Longitudinal ultrasound image corresponding to (B).
Hepatic veins. A. Transverse diagram, using a slightly cephalad angulation. The left, middle, and right hepatic veins can be imaged as they empty into the IVC just beneath the right diaphragm. B. Longitudinal diagram. The middle hepatic vein is shown as it empties into the IVC at the level of the right diaphragm. The main branch of the portal vein is seen in its extrahepatic location just superior to the head of the pancreas. The right renal artery is visualized posterior to the IVC. (C) Transverse ultrasound image corresponding to (A). (D) Longitudinal ultrasound image corresponding to (B).
Inferior Mesenteric Vein. Courses to the left of the superior mesenteric vein to join the splenic vein (Fig. 6-9). It is usually too small to visualize by ultrasound. Drains the left third and upper portion of the colon.
Inferior Vena Cava. Returns blood from the lower half of the body and enters the right atrium of the heart (Figs. 6-5, 6-6, and 6-8B). It is formed by the union of the iliac veins. A marked change in caliber can be appreciated with respiration (Fig. 6-10).
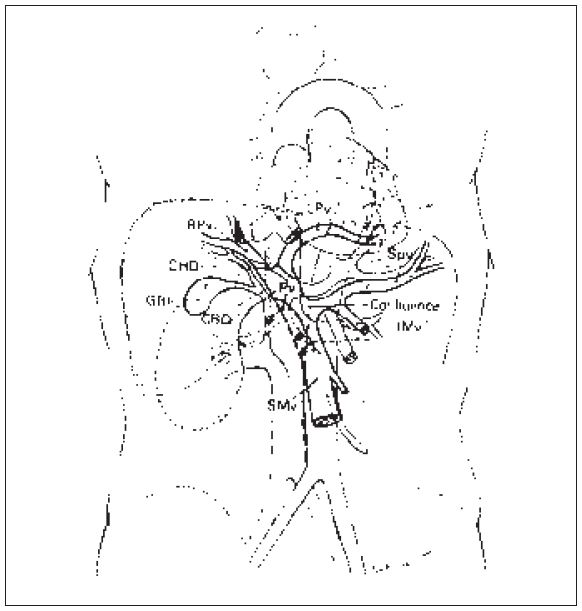
Figure 6-9. ![]() The splenic vein and superior mesenteric vein join (at the confluence) to form the main portal vein. The portal vein then branches into the liver, forming the left portal vein and the right portal vein.
The splenic vein and superior mesenteric vein join (at the confluence) to form the main portal vein. The portal vein then branches into the liver, forming the left portal vein and the right portal vein.
Left Renal Vein. Drains the left kidney. Runs anterior to the aorta and posterior to the superior mesenteric artery to enter the lateral wall of the IVC. (see Figs. 6-5, 6-6, and 6-12). The left renal vein is much longer than the right renal vein.
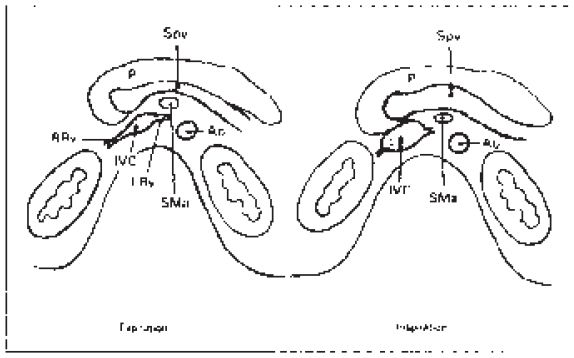
Figure 6-10. ![]() Venous structures should dilate at the end of deep inspiration or Valsalva maneuver. This maneuver can help confirm the venous nature of the vessels and enlarge the vessels to make it easier to image.
Venous structures should dilate at the end of deep inspiration or Valsalva maneuver. This maneuver can help confirm the venous nature of the vessels and enlarge the vessels to make it easier to image.
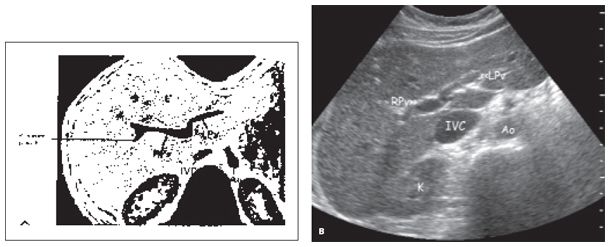
Figure 6-11. ![]() Transverse view within the liver. The portal vein branches into the left and right portal veins. The right vein again bifurcates the posterior branch supplying the posterior right lobe of the liver. A. Diagram. B. Ultrasound image.
Transverse view within the liver. The portal vein branches into the left and right portal veins. The right vein again bifurcates the posterior branch supplying the posterior right lobe of the liver. A. Diagram. B. Ultrasound image.
Main Portal Vein. Drains blood from the digestive tract and empties into the liver (Fig. 6-9). It is formed by the junction of the splenic vein and the superior mesenteric vein. The main portal vein divides into the left portal vein, which supplies blood to the left lobe of the liver (Fig. 6-9) and the right portal vein, which supplies the right lobe of the liver (Fig. 6-11). Portal veins characteristically run in triads with the hepatic arteries and bile ducts and branch away from the porta hepatis. They can be identified by their echogenic walls that occur due to acoustic reflection arising from the fibrous tissue that surrounds these triads.
Paraumbilical Vein. Courses along the falciform ligament. Connects the left portal vein to other collateral vessels near the umbilicus (Fig. 6-7). This vein is only seen in the setting of portal hypertension.
Right Renal Vein. Drains the right kidney and enters the lateral wall of the IVC (Figs. 6-5, 6-6, and 6-12).
Splenic Vein. Drains the spleen (Figs. 6-4, 6-5, and 6-9). It runs posterior to the pancreas and joins the superior mesenteric vein, thereby forming the main portal vein.
Superior Mesenteric Vein. Drains the cecum, transverse and sigmoid colon, and small bowel (Figs. 6-5, 6-9, and 6-12). Courses anterior to the IVC to join the splenic vein just next to the confluence behind the head of the pancreas.
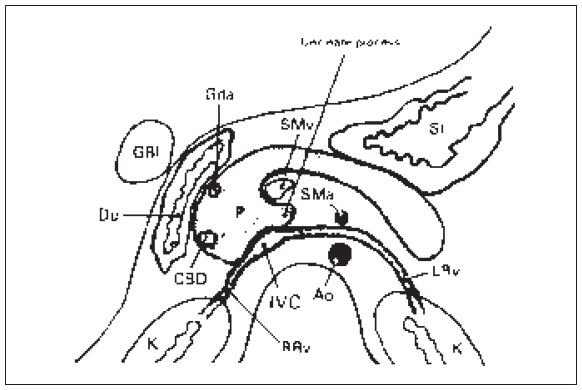
Figure 6-12. ![]() Many vascular structures can be visualized on a transverse section in the midabdomen. The IVC gives rise to the right and left renal veins; the latter passes between the aorta and the superior mesenteric artery. The superior mesenteric vein lies anterior to the IVC. The pancreas can be imaged anterior to these vessels. The gastroduodenal artery and the common bile duct assist in outlining the lateral margin of the head of the pancreas. When empty, the antrum walls of the stomach and the duodenum are seen as echo-free linear structures. The gallbladder is lateral to the duodenum.
Many vascular structures can be visualized on a transverse section in the midabdomen. The IVC gives rise to the right and left renal veins; the latter passes between the aorta and the superior mesenteric artery. The superior mesenteric vein lies anterior to the IVC. The pancreas can be imaged anterior to these vessels. The gastroduodenal artery and the common bile duct assist in outlining the lateral margin of the head of the pancreas. When empty, the antrum walls of the stomach and the duodenum are seen as echo-free linear structures. The gallbladder is lateral to the duodenum.
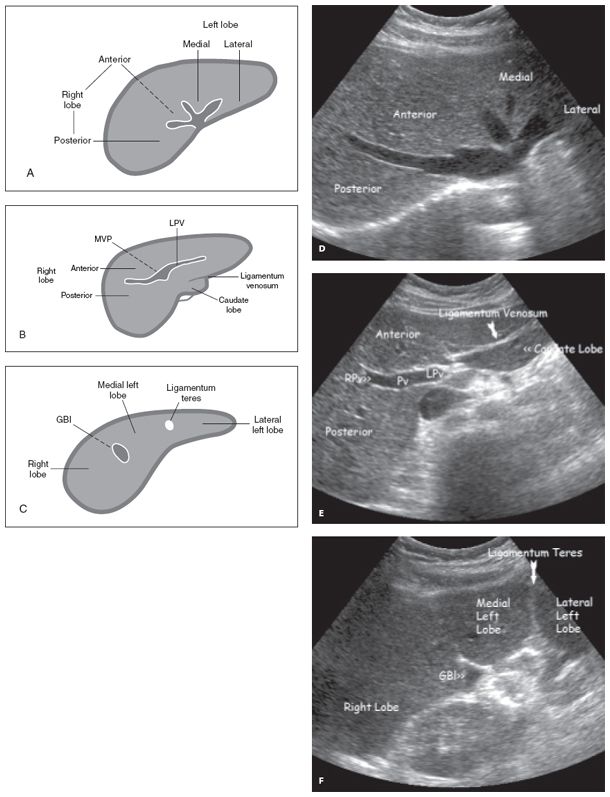
Figure 6-13. ![]() Series of transverse views of the liver to show vascular supply at different levels. Level A (diagram) and D (ultrasound image) are taken close to the diaphragm and show the hepatic veins. Level B (diagram) and E (ultrasound image) are taken in midliver and show the left and right portal veins. Level C (diagram) and F (ultrasound image) are taken at the level of the gallbladder.
Series of transverse views of the liver to show vascular supply at different levels. Level A (diagram) and D (ultrasound image) are taken close to the diaphragm and show the hepatic veins. Level B (diagram) and E (ultrasound image) are taken in midliver and show the left and right portal veins. Level C (diagram) and F (ultrasound image) are taken at the level of the gallbladder.
SONOGRAM ABBREVIATIONS
Crus of the Diaphragm. A tubular muscular structure seen anterior to the aorta and posterior to the IVC above the level of the celiac axis and superior mesenteric artery (Fig. 6-6). The right crus of the diaphragm arises from the lateral aspect of the first three lumbar vertebral bodies. The left crus arises from the first two lumbar vertebral bodies. Sonographically, the crus is seen as a thin hypoechoic band.
Ligamentum Teres. Echogenic structure within the left lobe of the liver, formed when the ductus venosus atrophies after birth. (Figs. 6-13 and 6-14).
Ligamentum Venosum. Echogenic line anterior to the caudate lobe and posterior to the left lobe of the liver (Figs. 6-13 and 6-14).
Main Lobar Fissure. Runs between the right and left lobes of the liver. Can be visualized between the gallbladder and the right portal vein (Fig. 6-14).
Porta Hepatis. Echogenic region where the portal vein, hepatic artery, and common bile duct enter the liver.
Splenic Hilum. Central area of the medial aspect of the spleen where vessels enter or exit.
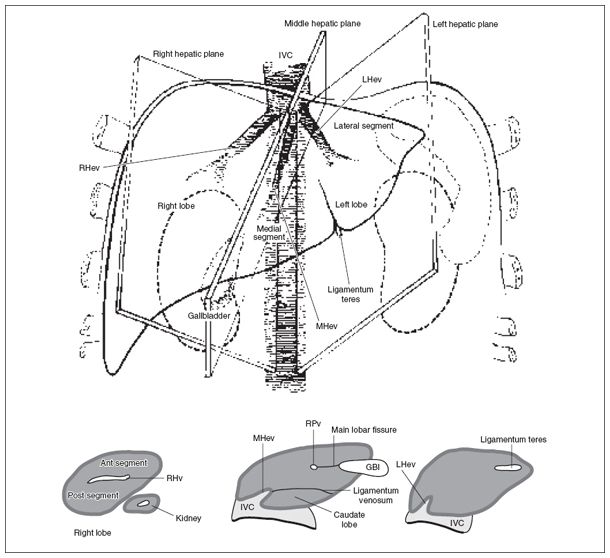
Figure 6-14. ![]() Diagram of the upper abdomen showing the liver, spleen, gallbladder, and kidneys. The hepatic veins represent the divisions between the lobes and segments of the liver. The middle hepatic vein divides the right and left lobes of the liver. The left hepatic vein separates the medial and lateral segments of the left lobe; the right hepatic vein separates the anterior and posterior segments of the right lobe of the liver. The gallbladder represents the inferior end of the separation between right and left lobes of the liver; the ligamentum teres represents the inferior end of the separation between the medial and lateral segments of the left lobe.
Diagram of the upper abdomen showing the liver, spleen, gallbladder, and kidneys. The hepatic veins represent the divisions between the lobes and segments of the liver. The middle hepatic vein divides the right and left lobes of the liver. The left hepatic vein separates the medial and lateral segments of the left lobe; the right hepatic vein separates the anterior and posterior segments of the right lobe of the liver. The gallbladder represents the inferior end of the separation between right and left lobes of the liver; the ligamentum teres represents the inferior end of the separation between the medial and lateral segments of the left lobe.
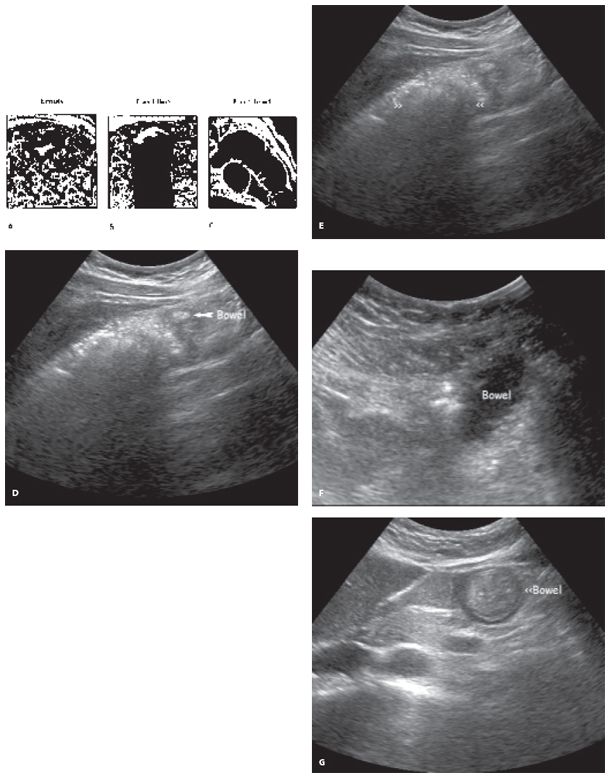
Figure 6-15. ![]() Bowel can have different sonographic appearances depending on its contents. A (diagram) and D (ultrasound image): When empty, there is a hypoechoic wall around an echogenic center. B (diagram) and E (ultrasound image): When gas-filled, there is acoustic shadowing. C (diagram) and F (ultrasound image): When fluid-filled, one may be able to make out the haustral markings of the colon or valvulae conniventes of the small bowel in the wall of the fluid-filled bowel. G (ultrasound image): bowel filled with echogenic fecal matter surrounded by hypoechoic bowel wall.
Bowel can have different sonographic appearances depending on its contents. A (diagram) and D (ultrasound image): When empty, there is a hypoechoic wall around an echogenic center. B (diagram) and E (ultrasound image): When gas-filled, there is acoustic shadowing. C (diagram) and F (ultrasound image): When fluid-filled, one may be able to make out the haustral markings of the colon or valvulae conniventes of the small bowel in the wall of the fluid-filled bowel. G (ultrasound image): bowel filled with echogenic fecal matter surrounded by hypoechoic bowel wall.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


