Fig. 3.1
Subtraction protocol. Injection of 12 MBq of 123I at T = -2h, injection of 740 of 99mTc-MIBI at T0, dual-tracer planar pinhole acquisition (20 min acquisition). 99mTc-MIBI pinhole planar image (left), 123I pinhole planar image (middle) and subtraction image (99mTc-MIBI-123I) (right). (a) Parathyroid adenoma located at the tip of the inferior pole of the left thyroid lobe (arrow). (b) Parathyroid adenoma located at the inner part of the right thyroid lobe (arrow). (c) Typical diffuse hyperplasia related to chronic renal failure (arrows)
3.1.8 SPECT/CT
3.1.8.1 Primary Hyperparathyroidism
SPECT/CT may provide improvement in sensitivity in comparison to single-tracer planar imaging, especially for posterior adenomas. In our opinion, the use of subtraction method using 123I and 99mTc-MIBI with pinhole planar acquisition (neck) followed by SPECT/CT (neck and mediastinum) is the most sensitive approach to detect and localise hyperfunctioning glands. SPECT can be performed as single tracer imaging or as a dual tracer technique with simultaneous acquisition (Figs. 3.2, 3.3 and 3.4). The energy windows for acquisition are the same as for planar and pinhole images [13, 40].
SPECT/CT provides the advantage over planar techniques to localise adenomas in the anterior-posterior plane [43, 44], offering critical information for surgeons. SPECT may reclassify apparently inferior adenomas (on planar images) to superior, P4-derived, adenomas prolapsed behind the lower pole of the thyroid gland. These adenomas can be located very deeply in the neck, in paraesophageal or in retroesophageal locations and may be missed by neck ultrasound (Figs. 3.2 and 3.3) [45]. By contrast, inferior glands are mostly located at the tip of the inferior pole of the thyroid lobe, in the thyrothymic tract or in the upper thymic horn and remain anterior on SPECT imaging (Fig. 3.4) [44]. These 3D information may also influence the surgical strategy such as resection via an endoscopic lateral approach for posterior adenomas (most often P4-derived) or a small cervical incision (mini-open approach) cervicotomy for P3-derived adenomas [46]. SPECT also enables a better localisation of ectopic glands (Fig. 3.3). The precise anatomic localisation of mediastinal adenomas provided by SPECT/CT may also influence the surgical strategy (mediastinoscopy /anterior mediastinotomy vs left thoracotomy) (Fig. 3.5).

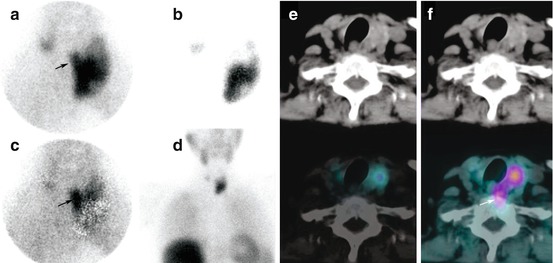
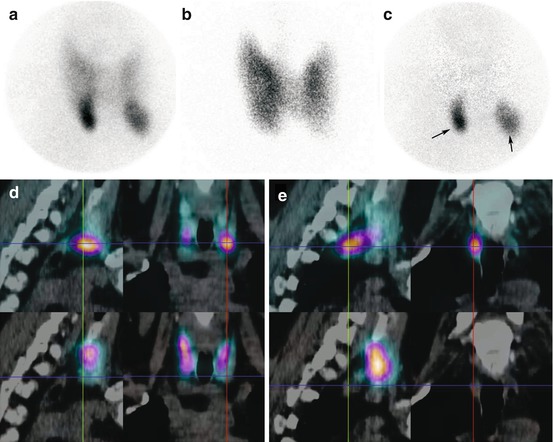
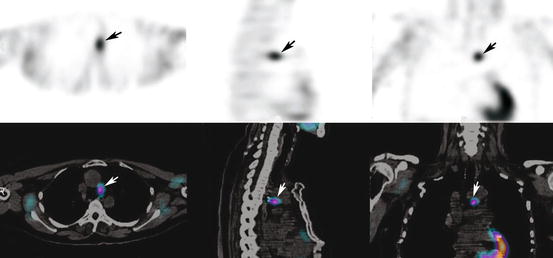
Fig. 3.2
P4 adenoma. (a) 99mTc-MIBI pinhole image, (b) 123I pinhole image, (c) substraction, (d) Dual isotope SPECT/CT images (99mTc-MIBI upper row; 123I lower row). Planar pinhole substraction images reveal a focal accumulation of 99mTc-MIBI located in the inner and lower pole of the right thyroid lobe. Note a right thyroid nodule on 123I scintigraphy. SPECT/CT demonstrates that the parathyroid gland is prolapsed behind the thyroid gland and is extended posteriorly (black arrows). This is a typical feature of P4 adenoma. Please note absence of 123I uptake in the parathyroid adenoma (lower row image)
Fig. 3.3
P4 adenoma. (a) 99mTc-sestaMIBI, (b) 123I, (c): substraction, (d) cervico-mediastinal acquisition, (e) CT and 123I SPECT/CT images, (f) CT and 99mTc- SPECT/CT images. Planar pinhole substraction images reveal a focal accumulation of 99mTc-MIBI located in the inner part of the left thyroid lobe (arrows). SPECT/CT demonstrates that the gland is prolapsed behind the thyroid gland and is extended posteriorly as almost all large P4 adenomas (white arrow). This patient had nodular thyroid disease with previous right thyroid lobectomy
Fig. 3.4
MEN1-related HPT. (a) 99mTc-MIBI, (b) 123I, (c) substraction, (d and e) Dual-isotope SPECT/CT images. Planar pinhole substraction images reveal two focal accumulation of 99mTc-MIBI located in the inferior poles of right and left thyroid lobes. SPECT/CT demonstrates a left P3 hyperfunctioning lesion (left arrow) (d) and a right P4 hyperfunctioning lesion prolapsed behind the thyroid gland (right arrow) (e). Please note absence of 123I uptake in the parathyroid lesions (lower row)
Fig. 3.5
Parathyroid adenoma in the aortopulmonary window (arrows). SPECT and SPECT/CT fusion images
Using a single-isotope protocol, SPECT/CT acquisitions are usually performed from 10 to 60 min after injection of 99mTc-MIBI [47–49]. Some teams acquire both early and late SPECT images. Iterative reconstruction methods are well suited to improve image quality. There is some evidence that early-phase SPECT or SPECT/CT imaging performs better than delayed imaging, presumably because of a rapid tracer wash-out in some hyperfunctioning glands [49–51] (Table 3.1). The use of SPECT/CT also provides an advantage over SPECT alone in patients with nodular goitre [53]. To minimise radiation exposure, the CT part of the SPECT/CT acquisition should probably be limited to the neck area in cases of absence of mediastinal foci on planar images [57].
Table 3.1
Performance of SPECT/CT in hyperparathyroidism
Authors | Disease | Numberof patients | SPECT/CT device | SPECT/CT protocol | Diagnostic performance | ||
|---|---|---|---|---|---|---|---|
Typeof analysis | Sensitivity | Specificity | |||||
Lavely et al. [49] | pHPT | 98 | Low-power CT | Early SPECT/CT | Per lesion | 62 | 99 |
– | – | – | – | Delayed SPECT/CT | – | 53 | 98 |
– | – | – | – | Early planar/delayed SPECT/CT | – | 61 | 98 |
– | – | – | – | Early SPECT/CT/delayed planar | – | 72 | 99 |
Patel et al. [52] | pHPT | 59 | Low-power CT | Early planar/delayed SPECT/CT | Per lesion | 90 | na |
Pata et al. [53] | pHPT + nodular goitre | 18 | SPECT alone | Early planar/delayed SPECT | Per neck quadrant | 56 | 62 |
– | – | 15 | Low-power CT | Early planar/delayed SPECT/CT | – | 87 | 87 |
Pata et al. [54] | pHPT | 27 | SPECT alone | Early planar/delayed SPECT | Per neck quadrant | 87 | 90 |
– | – | 28 | Low-power CT | Early planar/delayed SPECT/CT | – | 61 | 97 |
Ciappuccini et al. [55] | pHPT | 59 | Spiral CT | Early pinhole/delayed SPECT/CT | Per lesion | 92 | 83 |
Shafiei et al. [56] | pHPT + nodular goitre | 48 | Spiral CT | Early planar + SPECT/delayed planar | Per lesion | 67 | 87 |
– | – | – | – | Early planar + SPECT/CT/delayed planar | – | 78 | 97 |
Zhen et al. [57] | sHPT | 90 | Spiral CT | Early planar/delayed planar + SPECT/CT | Per patient | 79 | 100 |
3.1.8.2 Renal Hyperparathyroidism
SPECT/CT may increase sensitivity of single-tracer planar imaging [57] but probably have little impact on sensitivity in comparison to highly sensitive subtraction protocols using pinhole collimators [13] (Fig. 3.6). SPECT/CT is particularly helpful as a complement to planar imaging to pinpoint the position of mediastinal foci and other ectopic parathyroid glands [13].
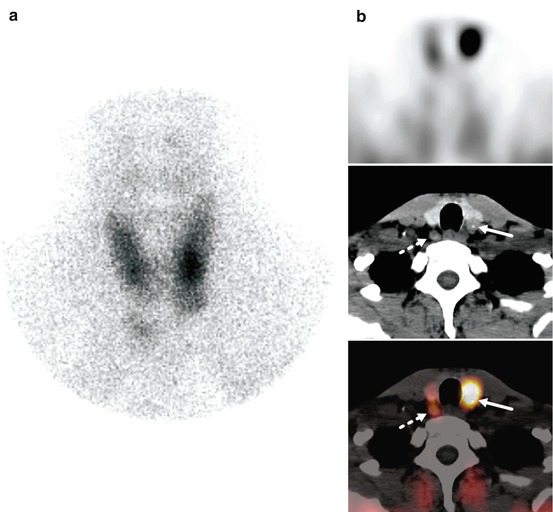
Fig. 3.6
Secondary hyperparathyroidism. (a) Early pinhole images and transaxial slices (b, from top to bottom: SPECT, CT and fused SPECT/CT slices) are shown. Whereas pinhole images show an intense focus on the left side, delayed SPECT/CT acquisition clearly shows a left parathyroid adenoma (arrow) and a second contralateral lesion at the same level, which harbours a low MIBI uptake (dotted arrow)
3.2 Benign Thyroid Disorders
3.2.1 Ectopic Thyroid Tissue
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


