Abstract
FDG-avid splenic lesions may be malignant (lymphoma most commonly) or benign, such as infections and sarcoid. Benign causes of splenic FDG avidity are common and must be distinguished from malignancy. FDG avidity of lymphoma tends to correlate with lymphoma grade; the higher the grade, the more FDG avid.
Keywords
FDG, PET/CT, spleen, lymphoma, sarcoid, splenic repopulation
When confronted with a focal splenic lesion, knowledge of the differential diagnosis for splenic masses is valuable ( Fig. 13.1 ). For malignancies of the spleen, lymphoma would be most common, whereas metastases are relatively uncommon and primary splenic malignancies are rare. Benign splenic lesions encountered on fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT) are common and include infections, sarcoidosis, and splenic repopulation.

Splenic Lymphoma
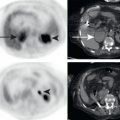
Lymphoma is by far the most common malignancy to involve the spleen. Splenic lymphoma may manifest as splenic enlargement (splenomegaly) or solitary or multifocal lesions. FDG avidity of lymphoma ranges from no apparent FDG avidity to markedly FDG avid. The extent of FDG avidity in lymphoma tends to correlate with pathologic rate. Lymphomas with maximum standarized uptake values (SUV) greater than 20 are most often high-grade lymphomas ( Fig. 13.2 ), whereas lymphomas with maximum SUV values less than 10 are most often low grade. This can be valuable in screening patients with low-grade lymphoma for transformation to higher-grade malignancy. Highly FDG-avid lesions would be the lesions to target for evaluation of possible high-grade malignancy. Low-grade lymphoma made be incidentally discovered during FDG PET/CT performed for another malignancy ( Fig. 13.3 ). If the FDG avidity of low-grade lymphoma nodes is low enough, they may not be readily apparent on the FDG PET images and must be appreciated by the enlarged lymph nodes on the corresponding CT images.