CHAPTER 11 Squamous Cell Carcinoma
Epidemiology
Tumors of the external auditory canal (EAC) are relatively uncommon. Squamous cell carcinoma represents the most common primary malignant tumor, followed by basal cell carcinoma and adenoid cystic carcinoma. The precise etiology of EAC carcinoma is unknown, but the majority of cases occur in patients with a long history of chronic inflammation of the EAC. Squamous cell carcinoma is encountered more commonly in females, and the median age of occurrence is 55 years.
Clinical Features
The diagnosis and staging of external canal cancer often present a significant challenge. There is usually a long delay that results from the similarity of its presentation with that of more commonly occurring benign inflammatory diseases, such as otitis externa or chronic otitis media, as well as the rarity of the disease. Early diagnosis, which is the single most important prognostic factor, is dependent on a high level of suspicion by the otolaryngologist. Persistent external otitis, despite routine treatment, should increase suspicion of carcinoma and prompt a biopsy. Persistent pain that is out of proportion to clinical abnormality or a change in pain pattern with a chronically painful ear should arouse suspicion. Pain is a common symptom and it often indicates underlying bone involvement. Bloody ear discharge is another hallmark of malignancy, although this is relatively rare. Advanced squamous cell carcinoma can invade adjacent structures, especially the middle ear cleft and parotid gland. Facial weakness may indicate the involvement of cranial nerve VII.
Pathology
External auditory canal carcinomas may appear as polypoidal lesions on clinical inspection. The EAC cartilage does not provide an efficient barrier against tumor spread, and permits radial spread of malignancy. Anteriorly located dehiscences (the fissures of Santorini) and bony-cartilaginous junctions can allow the tumor direct access to the periparotid tissues and temporomandibular joint.
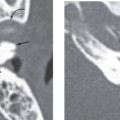
Tumor growth medially along the external ear canal can involve the tympanic membrane and bony tympanic ring, allowing subsequent invasion into the middle ear. Spread into the otic capsule is less common, as dense bone of the otic capsule provides a more effective barrier against tumor spread.
The facial nerve and the stylomastoid foramen serve as metastatic routes to the soft tissues of the neck and the parotid. Proximal extension of malignant cells along the facial nerve (retrograde perineural spread) carries the tumor toward inner ear and posterior fossa.
Nodal metastasis is encountered in advanced malignancies and can be seen in 8 to 10% of cases. The lymphatic drainage of the auricle and EAC extends anteriorly to the periparotid lymph nodes and parotid gland. Drainage to the jugular chain or mastoid group of nodes may also occur.
Treatment
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


