Systemic Nodal Metastases in Neck
Patricia A. Hudgins, MD
Key Facts
Terminology
Cervical metastatic adenopathy from infraclavicular primary tumor
Virchow node is left supraclavicular nodal metastasis
Imaging
Nodes generally in lower neck, especially on left
Variable size nodes, often > 1.5 cm
May be cluster of small nodes
May form conglomerate mass > 5-6 cm
Calcification may be evident on CT when primary tumor is adenocarcinoma
Top Differential Diagnoses
Reactive lymph nodes
Sarcoidosis nodes
SCCa metastatic nodes
Non-Hodgkin lymphoma nodes
Pathology
Esophageal, breast, and lung malignancies are most common primary tumors
May be unknown primary tumor
Focal nonenhancement on CT/MR corresponds to nest of tumor cells or necrosis
Clinical Issues
Systemic neck metastases less common than head and neck SCCa nodes
Diagnostic Checklist
If patient presents with nodal mass, 1st look for head and neck primary tumor
If infrahyoid nodal metastasis, suspect systemic primary tumor
When neck nodes are calcified, suspect thyroid primary or systemic adenocarcinoma
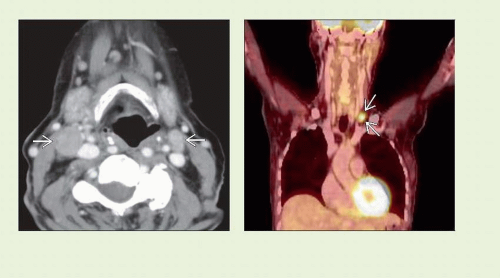 Figure 1 (Left) Axial CECT shows enlarged, noncalcified, solidly enhancing bilateral level IIA neck nodes  . No primary source was evident in neck, but patient was found to have primary lung carcinoma. (Right) Coronal PET/CT in a patient with ovarian carcinoma reveals a single enlarged left supraclavicular node . No primary source was evident in neck, but patient was found to have primary lung carcinoma. (Right) Coronal PET/CT in a patient with ovarian carcinoma reveals a single enlarged left supraclavicular node  with FDG avidity. The patient had been previously treated for abdominal metastases and had known pulmonary metastases at the time of study. with FDG avidity. The patient had been previously treated for abdominal metastases and had known pulmonary metastases at the time of study. |
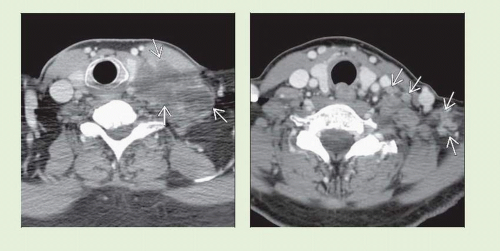 Figure 1 (Left) Axial CECT shows large complex conglomerate left supraclavicular nodal mass
 with extensive necrosis & infiltration of scalene and sternocleidomastoid muscles. Patient had neural deficits from invasion of brachial plexus. Fine needle aspiration revealed metastatic colonic adenocarcinoma. (Right) Axial CECT reveals multiple small nodes with extensive necrosis & infiltration of scalene and sternocleidomastoid muscles. Patient had neural deficits from invasion of brachial plexus. Fine needle aspiration revealed metastatic colonic adenocarcinoma. (Right) Axial CECT reveals multiple small nodes  in lower left neck in a patient with known metastatic breast carcinoma. Nodes are heterogeneous, many with focal eccentric low density, indicating necrosis. in lower left neck in a patient with known metastatic breast carcinoma. Nodes are heterogeneous, many with focal eccentric low density, indicating necrosis.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|