Abstract
Temporal bone fractures are divided into longitudinal and transverse fractures, each with their particular clinical features. Transverse fractures mainly cause conductive hearing loss, whereas longitudinal fractures almost invariably cause sudden deafness often associated with vertigo. Facial nerve paralysis is most often associated with longitudinal fractures.
Imaging is regarded crucial in temporal bone fractures. A comparison of both temporal bones and knowledge of the normal temporal bone anatomy, sutures, and fissures are of utmost importance to recognize fractures. It should be kept in mind that delayed imaging in the case of transverse fractures is often required, as the associated middle ear and mastoid blood deposition may obscure ossicular dissociation in the beginning, clinically as well as on imaging.
Cone beam CT is to be preferred over CT for the evaluation of temporal bone fractures because of its lower radiation doses and higher resolution. Double oblique reconstructions are mandatory for the evaluation of eventual ossicular disruption and/or dissocation. In the case of a transverse fracture, MRI is obligatory to evaluate the status of the membranous labyrinth. The types of fractures and their complications are extensively illustrated in this chapter.
Keywords
Ear, inner, Ear, middle, Hearing loss, conductive, Hearing loss, sensorineural, Skull fracture, Temporal bone
Temporal Bone Pseudofractures—Fracture Mimics
An important challenge in detecting and classifying temporal bone fractures is the inherent complexity of the temporal bone anatomy. Although the evaluation of symmetry is helpful to distinguish normal anatomy from acute injury, temporal bone sutures or fissures and canals can still be wrongly interpreted as fractures.
The temporal bone has a complex structure. It is a part of the lateral wall of the skull and forms an important part of the skull base.
The temporal bone consists of five parts: squamous, mastoid, petrous, tympanic, and styloid parts.
There are so-called external fissures or sutures that separate the temporal bone from its neighboring skull bones.
These include the sphenosquamosal suture, formed by the greater wing of the sphenoid and the squamous temporal bone, located lateral to the foramen spinosum ( Fig. 7.1A ).

The occipitomastoid suture separates the mastoid process from the occipital bone ( Fig. 7.1A ).
The sphenopetrosal suture, which courses anteromedially along the anterior margin of the petrous bone, between the foramen ovale and the carotid canal, contains the deeper petrosal nerve ( Fig. 7.1B ).
The petrooccipital suture also runs anteromedially, coursing superior to the sphenopetrosal suture and along the posterior aspect of the temporal bone, posterior to the carotid canal ( Fig. 7.1B ).
The five portions of the temporal bone are separated by several internal sutures and fissures.
The tympanosquamous and tympanomastoid fissures run parallel to the anterior and posterior walls of the external auditory canal, respectively. Of these two, the tympanosquamous fissure, being the most anterior one, is more consistently seen and more likely to be mistaken for an external auditory canal fracture ( Fig. 7.2 ). It follows the tympanosquamous fissure medially and divides to form the petrosquamosal and petrotympanic fissures.

The tympanomastoid fissure runs posterior and parallel to the external auditory canal ( Fig. 7.2 ).
The petrosquamosal fissure is occasionally seen on axial images extending anteromedially from the mandibular fossa toward the greater wing of the sphenoid ( Fig. 7.2 ).
The petrotympanic fissure is best seen on sagittal images as a short-segment channel connecting the upper tympanic cavity with the mandibular fossa.
There are also intrinsic channels or canals that might be mistaken for a fracture.
These include the cochlear aqueduct, the glossopharyngeal sulcus, the vestibular aqueduct, the singular nerve canal, the subarcuate canal, the mastoid canaliculus, the inferior tympanic canaliculus, the canal for the chorda tympani, and the groove for the superior petrosal sinus.
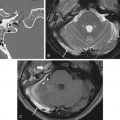
The cochlear aqueduct contains perilymph and is obliquely oriented. It extends from the subarachnoid space to the region close to the round window membrane. The medial aspect of the cochlear aqueduct is funnel shaped and almost invariably visible. Its lateral part is usually very thin ( Fig. 7.3A ).

It runs in the same direction as the internal auditory canal, but in a lower position in the temporal bone and is usually much thinner. Its size and delineability can be variable.
The glossopharyngeal sulcus represents the point of entry of the glossopharyngeal nerve into the pars nervosa of the jugular foramen. It is consistently seen on axial images a few millimeters below the cochlear aqueduct ( Fig. 7.3B ).
The vestibular aqueduct contains the endolymphatic duct and sac, which allows passage of endolymph. It runs from the vestibule to the posterior surface of the temporal bone, parallel and posterior to the posterior semicircular canal. Again, its size and delineability can be variable ( Fig. 7.4 ).

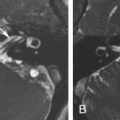
The singular canal carries the singular or posterior ampullary nerve. It extends from the posterior inferior wall of the fundus of the internal auditory canal to the junction of the vestibule with the ampulla of the posterior semicircular canal ( Fig. 7.5A ).

The subarcuate canal is a dura-lined canal for the subarcuate artery, which has an anterior convex course between the two limbs of the superior semicircular canal ( Fig. 7.5B ). It is prominent in children, in contrast to adults, where it is significantly reduced in size.
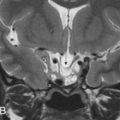
The mastoid canaliculus contains the nerve of Arnold, a branch of the 10th cranial nerve, and can be seen as a linear canal connecting the jugular foramen with the mastoid segment of the facial nerve canal ( Fig. 7.6A ).

The inferior tympanic canaliculus contains the inferior tympanic branch, also called Jacobson nerve. It runs from the spina in the jugular foramen between the pars vascularis and pars nervosa upward to the middle ear and can be evaluated on coronal ( Fig. 7.6B–E ) as well as on axial images.
A glomus jugulare tumor extends along this pathway from the jugular foramen toward the middle ear cavity. It also forms the point of entry of the aberrant internal carotid artery, when present.
The canal for the chorda tympani runs from the third or mastoid segment of the facial nerve upward, laterally and anteriorly to the middle ear cavity where it runs through the middle ear just medial to the tympanic membrane. It can be evaluated in the axial ( Fig. 7.7A–D ) as well as in the coronal planes ( Fig. 7.7E–G ).


The groove for the superior petrosal sinus is a deep groove that runs on the upper edge of the petrosal pyramid in which the superior petrosal vein runs ( Fig. 7.8 ). The depth of the groove may be variable, and the superior semicircular canal may be dehiscent into the sinus.

Temporal Bone Fractures
Temporal bone fractures have been traditionally classified as longitudinal or transverse, reflecting the relationship of the fracture line with regard to the long axis of the petrous bone.
Longitudinal fractures form the majority of the fractures. They are caused by a temporoparietal blow on the head, and the forces are diverted along the long axis of the temporal bone. Longitudinal fractures comprise 70%–90% of the temporal bone fractures and extend anteromedially, often involving the external auditory canal and the middle ear cavity ( Fig. 7.9 ).

The ossicles are frequently involved with subsequent conductive hearing loss. Evaluation of ossicular damage is best done using CT or cone beam CT (CBCT) after resorption of the hemotympanum, as the opacification caused by the blood in the middle ear might obscure subtle ossicular dislocations ( Fig. 7.10 ).

Related posts:
 Imaging in Endoscopic Endonasal Skull Base Surgery
Imaging in Endoscopic Endonasal Skull Base Surgery
 Imaging of the Postoperative Middle Ear, Mastoid, and Internal Auditory Canal
Imaging of the Postoperative Middle Ear, Mastoid, and Internal Auditory Canal
 Imaging of the Facial Nerve
Imaging of the Facial Nerve
 Jugular Foramen
Jugular Foramen
 Skull Base Bone Lesions I: Imaging Technique, Developmental and Diffuse Bone Lesions
Skull Base Bone Lesions I: Imaging Technique, Developmental and Diffuse Bone Lesions
 Skull Base Bone Lesions II: Benign and Malignant Tumors
Skull Base Bone Lesions II: Benign and Malignant Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


