Temporomandibular Joint
Jeffrey J. Peterson
Thomas H. Berquist
▪ ANATOMY
KEY FACTS
The temporomandibular joint (TMJ) is a synovial joint divided by a disc into superior and inferior compartments.
The normal disc is biconcave.
The posterior band is thicker and separated from the anterior band by the thin intermediate zone, giving the disc a “bow-tie” configuration.
The posterior attachment (bilaminar zone) contains the neurovascular supply for the disc.
When the mouth is closed, the disc is at the apex of the mandibular condyle.
With opening of the mouth, the mandibular condyle translates forward.
The normal disc remains centered over the condyle as the mouth opens.
 FIGURE 1-1. Normal temporomandibular joint (TMJ) in the sagittal (A) and coronal (B) planes. |
▪ INTERNAL DERANGEMENT
KEY FACTS
The disc is normally at the 12-o’clock position, with the mouth in the closed position. There is some degree of displacement in up to 34% of asymptomatic patients.
Internal derangement is defined as an abnormal relationship or position of the disc to the condyle and articular eminence.
The cause is unknown, but trauma, malocclusion, bruxism, hypermotility, ligament laxity, condylar abnormalities, and stress are implicated.
Females outnumber males by a ratio of 5:1.
Internal derangement is a progressive process.
Initially anterior, medial, or lateral displacement occurs when the mouth is closed, which reduces with opening.
The disc no longer reduces as elasticity decreases.
The disc becomes deformed with secondary bony changes.
Anterior displacement is most common, and 80% to 90% are bilateral. Medial or lateral displacement occurs in 5%, and posterior displacement occurs in 1%.
Clinical symptoms include pain, clicking, and reduced motion.
 FIGURE 1-2. Disc displacement categories: normal (A), anterior displacement (B), partial anterior displacement in lateral joint (C), partial anterior displacement in medial joint (D), rotational anterolateral displacement (E), rotational anteromedial displacement (F), lateral displacement (G), medial displacement (H), and posterior displacement (I). |
SUGGESTED READING
Aiken A, Bouloux G, Hudgins P. MR imaging of the temporomandibular joint. Mag Reson Imaging Clin N Am. 2012;20(3):397-412.
Milano V, Desiate A, Bellin R, et al. Magnetic resonance imaging of temporomandibular disorders: classification, prevalence, interpretation of disc displacement and deformation. Dentomaxillofac Radiol. 2000;29:353-361.
Sale H, Bryndahl F, Isberg A. Temporomandibular joints in asymptomatic and symptomatic volunteers: a prospective 15-year follow-up clinical and MR imaging study. Radiology. 2013;267(1):183-194.
▪ ANTERIOR DISC DISPLACEMENT
KEY FACTS
Anterior disc displacement occurs most commonly; 80% to 90% are bilateral.
Ninety percent of nondeformed anteriorly displaced discs reduce with opening.
Seventy-six percent of distorted discs do not reduce with opening.
Symptoms increase as disc deformity progresses.
Secondary signs of internal derangement.
Joint effusion
Joint space asymmetry
Marrow edema
Condylar erosion
Lateral pterygoid abnormalities
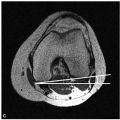
 FIGURE 1-3. (A) Schematic diagrams depicting anterior disc displacement without (left) and with (right) reduction. Sagittal T1-weighted magnetic resonance (MR) images show the normal imaging appearance of the disc (arrowhead) with open-mouth position (B) and closed-mouth positioning (C). Anterior disc dislocation without reduction (arrowhead) seen with open-mouth (D) and closed-mouth positioning (E). Anterior disc dislocation with reduction (arrowhead) seen with open-mouth (F) and closed-mouth positioning (G). |
 FIGURE 1-3. (continued)
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|