Pelvis, Hips, and Thighs
Daniel E. Wessell
Jeffrey J. Peterson
Thomas H. Berquist
▪ TRAUMA: PELVIC FRACTURES—MINOR
KEY FACTS
Mechanism of injury—fall or minor trauma
Usually older age group
Fractures of individual bones or single break in pelvic ring
Minor fractures account for 25% of pelvic fractures
Common minor fractures
Avulsion fractures (Fig. 3-1)
Traumatic and apophyseal in adolescents
Pathologic in the older age group
Ischial fractures
Pubic rami fractures
Transverse sacral fractures (up to 70% missed on routine radiographs)
Complications—pain, rarely significant complications compared with complex fractures
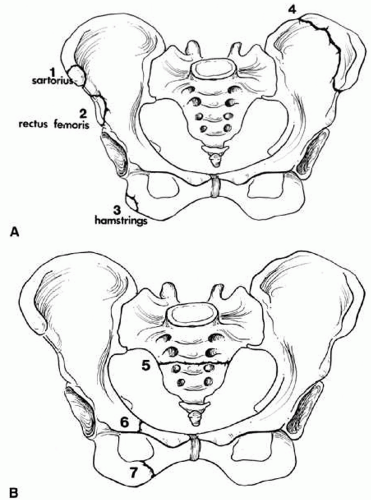 FIGURE 3-1. Common minor fractures of the pelvis. (A) Anterior superior iliac spine (1), anterior inferior iliac spine (2), ischial tuberosity (3), and iliac wing (4); 1 to 3 are avulsion injuries with muscles labeled. (B) Transverse sacral fracture (5) and isolated pubic rami fractures (6 and 7). |
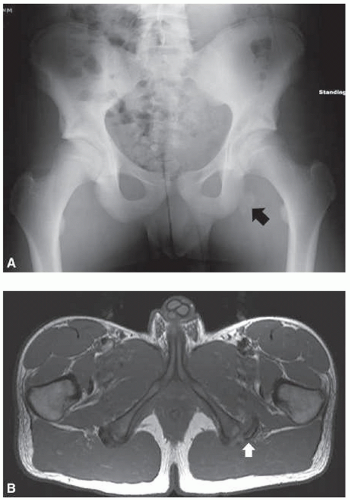 FIGURE 3-2. (A) Anteroposterior (AP) radiograph of the pelvis demonstrating a left ischial tuberosity avulsion fracture (black arrow). (B) Axial T1-weighted magnetic resonance (MR) image of the same patient redemonstrates the fracture (white arrow). |
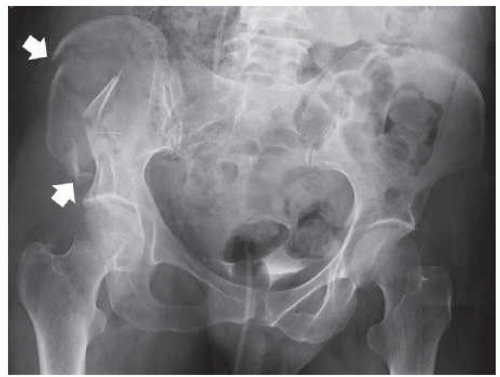 FIGURE 3-3. Anteroposterior (AP) pelvis radiograph demonstrating an isolated comminuted right iliac wing fracture (white arrows). |
SUGGESTED READING
Bui-Mansfield LT, Chew FS, Lenchik L, et al. Nontraumatic avulsions of the pelvis. Am J Roentgenol. 2002;178:423-427.
Singer G, Eberl R, Wegmann H, et al. Diagnosis and treatment of apophyseal injuries of the pelvis in adolescents. Semin Musculoskelet Radiol. 2014;18(5):498-504.
Young JWR, Resnick C. Fractures of the pelvis: current concepts in classification. Am J Roentgenol. 1990;155:1169-1175.
▪ TRAUMA: PELVIC FRACTURES—SINGLE BREAK IN PELVIC RING
KEY FACTS
Mechanism of injury—minor trauma
Usually nondisplaced pubic rami fractures involving one side
Account for approximately one-third of pelvic fractures
Complications—pain, local hematoma
Magnetic resonance (MR) may detect unsuspected posterior ring injuries
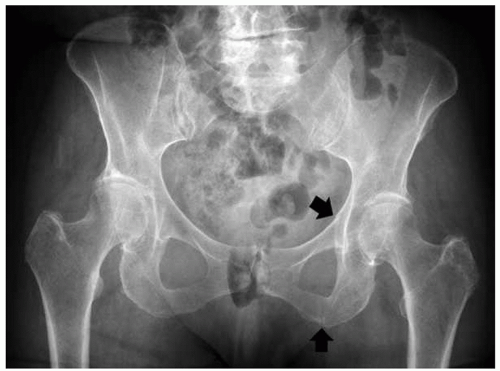 FIGURE 3-4. Anteroposterior (AP) pelvis radiograph demonstrating minimally displaced left superior and inferior pelvic rami fractures (black arrows) resulting in a single break in the pelvic ring. |
SUGGESTED READING
Berquist TH. Imaging of Orthopedic Trauma. 2nd ed. New York: Raven Press; 1992:207-310.
Cosker TDA, Ghandour A, Gupta SK, et al. Pelvic ramus fractures in the elderly: 50 patients studied with MRI. Acta Orthop. 2005;76:513-516.
Mucha P, Farnell MB. Analysis of pelvic fracture management. J Trauma. 1984;24:379-386.
▪ TRAUMA: PELVIC FRACTURES—COMPLEX
KEY FACTS
Mechanism of injury—high-velocity trauma, such as a motor vehicle accident
Lateral compression (41% to 72% of cases)
Anteroposterior (AP) compression (15% to 25% of cases)
Vertical shearing injuries (6% of cases)
Combined mechanisms (14% of cases)
Two or more breaks in the pelvic ring
Occur in younger age group (52% are less than 30 years of age)
Complications may be severe 100% result from multiple complications.” class=HASTIP>*
Hemorrhage
71%
Other associated fractures
65%
Genitourinary
22%
Neural injury
21%
Head injury
11%
Chest injury
11%
Abdomen injury
11%
Additional imaging, specifically computed tomography (CT), is usually required to define extent of injury
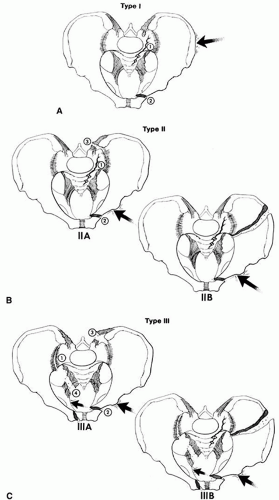 FIGURE 3-5. Lateral compression injuries. (A) Type I: force applied posterolaterally (arrow), resulting in a crush injury to the sacrum, ilium, and sacroiliac joint (1) and oblique or horizontal pubic rami fractures (2). (B) Type II: force directed anterolaterally (arrow), resulting in diastasis of the sacroiliac joint (1 and 3) (Type IIA) or iliac wing fracture (Type IIB) plus oblique or horizontal pubic rami fractures (2). (C) Type III: force applied anterolaterally (arrow) with oblique or horizontal pubic rami fractures (2) and involvement of both sacroiliac joints and ligaments (1, 3, and 4) (Type IIIA) or sacroiliac joints and ipsilateral iliac wing fracture (Type IIIB). |
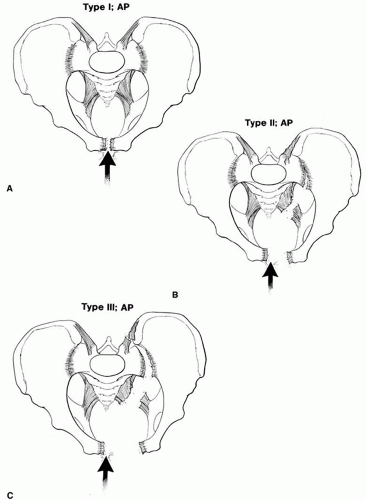 FIGURE 3-6. Anteroposterior (AP) compression injuries. (A) Type I AP compression injury with vertical pubic rami fractures. Sacroiliac joints are normal. Note the elevated bladder resulting from a large pelvic hematoma. (B) Type II: wider diastasis of the pubic symphysis or vertical pubic rami fractures with disruption of the anterior sacroiliac ligaments. (C) Type III: wider diastasis of the pubic symphysis or displaced vertical pubic rami fractures with disruption of both the anterior and posterior sacroiliac ligaments. (D) AP compression injury with vertical pubic rami fractures. Sacroiliac joints are normal. Note the elevated bladder resulting from a large pelvic hematoma (Type I). (E) AP pelvis radiograph demonstrating a Type II AP compression injury with diastasis of the pubic symphysis, and widening of the anterior right sacroiliac joint (white arrow). |
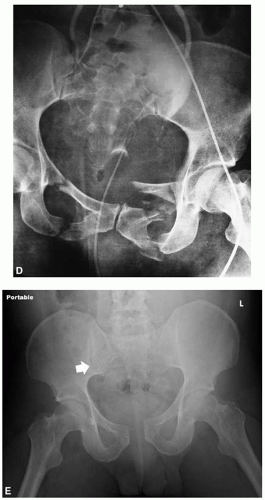 FIGURE 3-6. (continued) |
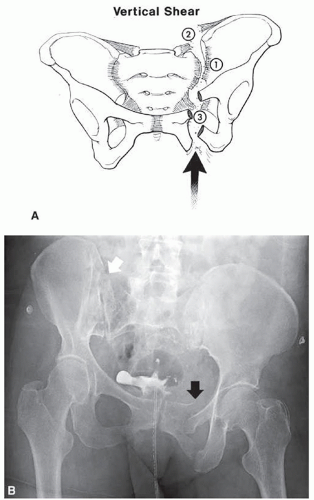 FIGURE 3-7. Vertical shearing injury. (A) Force is applied vertically (arrow) with vertical pubic rami fractures (3) or step-off at the pubic symphysis and disruption of the anterior and posterior sacroiliac ligaments (1 and 2). (B) Anteroposterior (AP) pelvis radiograph demonstrating widening and step-off of the right sacroiliac joint (white arrow) and vertically displaced left pelvic rami fractures (black arrow). Contrast and catheter in bladder from computed tomography (CT) cystogram to evaluate for bladder injury. |
SUGGESTED READING
Failinger S, McGarrity PL. Unstable fractures of the pelvic ring. J Bone Joint Surg. 1992;74A:781-791.
Khurana B, Sheehan SE, Sodickson AD, et al. Pelvic ring fractures: what the orthopedic surgeon wants to know. Radiographics. 2014;34(5):1317-1333.
Young JWR, Resnick C. Fractures of the pelvis: current concepts and classification. Am J Roentgenol. 1990;155:1169-1175.
▪ TRAUMA: ACETABULAR FRACTURES—SIMPLE
KEY FACTS
Mechanism of injury—lower extremity trauma with force directed to the femoral head.
Fractures involve posterior acetabulum if hip flexed. Posterior dislocation may occur.
Transverse and anterior fractures occur with lateral blow to greater trochanter.
AP and Judet views may detect injury. CT with coronal and sagittal reformatting is useful to evaluate and characterize subtle fractures and the joint space involvement.
Complications—minor, or arthrosis in later years.
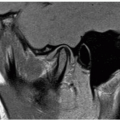
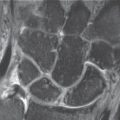
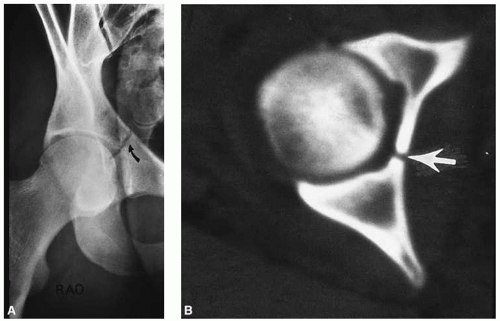 FIGURE 3-8. (A) Judet view of the hip demonstrating a nondisplaced central acetabular fracture (curved arrow). (B) Computed tomography (CT) image demonstrating an uncomplicated central acetabular fracture (arrow). |
SUGGESTED READING
Durkee NJ, Jacobson J, Jamadar D, et al. Classification of common acetabular fractures: radiographic and CT appearances. Am J Roentgenol. 2006;187:915-925.
Letournel E. Acetabular fracture classification and management. Clin Orthop. 1980;151:81-106.
▪ TRAUMA: ACETABULAR FRACTURES—COMPLEX
KEY FACTS
Multiple fracture classification systems have been proposed.
Two-column, transverse with posterior wall involvement, and posterior wall fractures account for 66% of acetabular fractures. “T” and transverse fractures are the next two most common injury patterns. These five patterns account for 90% of acetabular fractures.
Definition of extent of articular and anterior and posterior column involvement is critical for treatment planning.
CT with reformatting in sagittal and coronal planes, or three-dimensional volume rendering, or shaded surface display is essential.
Complications are similar to complex pelvic fractures (see section on Pelvic Fractures—Complex).
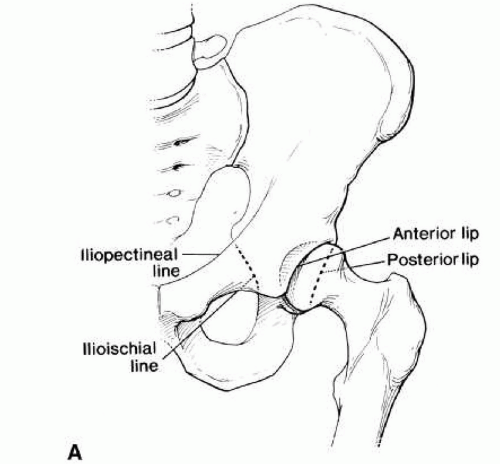 FIGURE 3-9. (A) Acetabular margins and the anterior (iliopectineal) and posterior (ilioischial) columns. (B, C) Three-dimensional shaded surface displays computed tomography (CT) images of the pelvis with electronic subtraction of the right femur demonstrating the anterior (A) and posterior columns (P). Images are obtained with 45-degree right posterior obliquity (B) and left posterior obliquity (C) like the Judet radiographic views of the pelvis. |
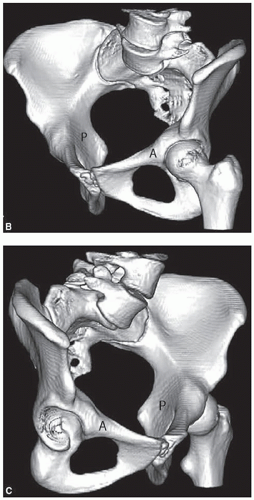 FIGURE 3-9. (continued) |
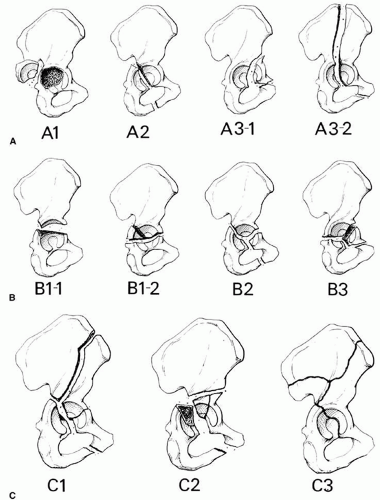 FIGURE 3-10. Fracture patterns (AO classification). (A) Type A: A1, posterior wall fracture; A2, posterior column fracture; A3-1, anterior wall fracture; A3-2, anterior column fracture. (B) Type B1-1, transverse fracture; Type B1-2, transverse with posterior wall fracture; Type B2, fracture; Type B3, anterior column with posterior transverse fracture. (C) Type C1, both columns with fracture extending to the iliac crest; Type C2, both columns extending to anterior inferior iliac spine; Type C3, both columns with extension to sacroiliac joint. Types A1, B1-1, B1-2, B-2, and C1 are the most common. |
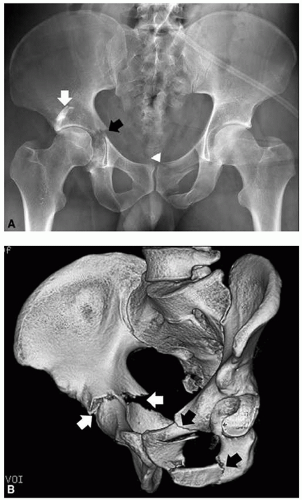 FIGURE 3-11. Complex acetabular fracture. (A) Anteroposterior (AP) pelvis radiograph shows a displaced right transverse acetabular fracture (black arrow), a displaced right posterior wall fracture (white arrow), and left superior and inferior pelvic rami fractures (white arrowhead). (B, C) Three-dimensional shaded surface displays computed tomography (CT) images of the fractures. The right posterior oblique view (B) demonstrates the transverse acetabular fracture (white arrows) and the pelvic rami fractures (black arrows). The posterior view (C) demonstrates the transverse acetabular fracture (white arrow) and the posterior wall fracture (black arrow). |
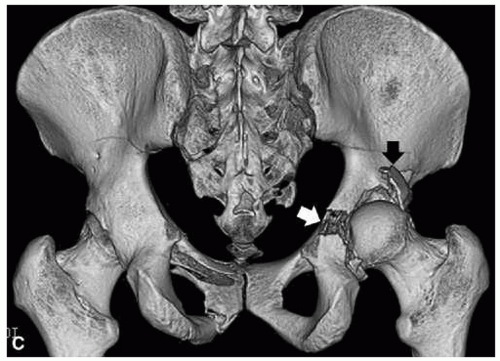 FIGURE 3-11 (continued) |
SUGGESTED READING
Brandser E, Marsh JL. Acetabular fractures: easier classification with a systematic approach. Am J Roentgenol. 1998;171:1217-1228.
Saks BJ. Normal acetabular anatomy for acetabular fracture assessment: CT and plain film correlation. Radiology. 1986;159:139-145.
Scheinfeld MH, Dym AA, Spektor M, et al. Acetabular fractures: what radiologists should know and how 3D CT can aid classification. Radiographics. 2015;35:555-577.
▪ TRAUMA: FRACTURE/DISLOCATION—DISLOCATION OF THE HIP
KEY FACTS
Hip dislocations account for 5% of all skeletal dislocations.
Mechanism of injury—high-velocity trauma, usually in young adults
Posterior dislocations—10 times more common than anterior. Compressive force to foot or knee with hip flexed. Posterior acetabular fractures are common.
Anterior dislocations—forced abduction and external rotation. Femoral head and anterior acetabular fractures are common.
Up to 75% have multiple other injuries.
Most complete dislocations are obvious on the AP view of pelvis or involved hip.
CT is useful for complete evaluation of the joint space and associated fractures, especially after reduction.
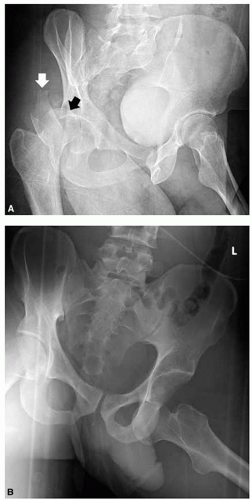 FIGURE 3-12. (A) Left posterior oblique (Judet) radiograph demonstrates posterior dislocation of the right femoral head (black arrow) and a posterior wall acetabular fracture (white arrow). (B) Anteroposterior (AP) pelvic radiograph demonstrates an anterior dislocation of the left femoral head. |
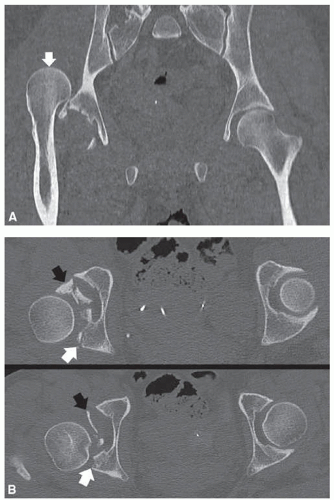 FIGURE 3-13. (A) Coronal multiplanar reformat computed tomography (CT) image of a posterior dislocation. Note the posterosuperior position of the femoral head (white arrow), which is typical. (B) Two axial CT images after attempted reduction of the posterior dislocation shown in (A). Multiple intra-articular fragments (black arrows) from the posterior wall fracture (white arrows) are preventing reduction. |
SUGGESTED READING
Pfeifer K, Leslie M, Menn K et al. Imaging findings of anterior hip dislocations. Skeletal Radiol. 2017; doi:10.1007/s00256-017-2605-x
Richardson P, Young JWR, Porter D. CT detection of cortical fracture of the femoral head associated with posterior dislocation of the hip. Am J Roentgenol. 1990;155:93-94.
Rosenthal RE, Coher WL. Fracture dislocations of the hip: an epidemiologic review. J Trauma 1979;19:572-581.
▪ TRAUMA: FEMORAL NECK FRACTURES
KEY FACTS
Occur in the elderly and in females more than in males
Mechanism of injury—minimal trauma or fall
Garden classification
Type I: incomplete involving lateral cortex
Type II: complete, but undisplaced
Type III: partially displaced
Type IV: completely displaced
Some prefer undisplaced (Types I and II) and displaced (Types III and IV)
Imaging of subtle undisplaced fractures may require magnetic resonance imaging (MRI) for detection. Displaced fractures usually are obvious on routine radiographs
Complications
Mortality: 10% to 20% in the first 30 days after injury and surgery
Mortality: approximately 30% first year after injury
Avascular necrosis (AVN) is common with displaced fractures
Treatment—pin undisplaced and endoprostheses used for displaced fractures because of high incidence of AVN
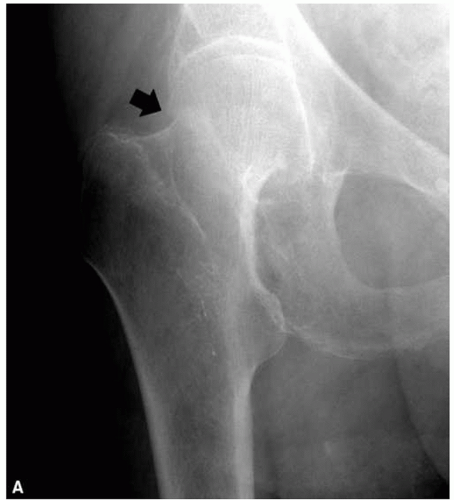 FIGURE 3-14. (A) Anteroposterior (AP) right hip radiograph demonstrates an impacted femoral neck fracture (black arrows) with cortical disruption and trabecular compression laterally. (B) Treated by percutaneous pinning. |
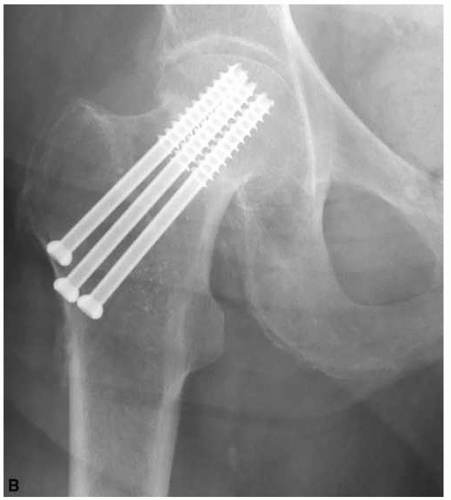 FIGURE 3-14 (continued) |
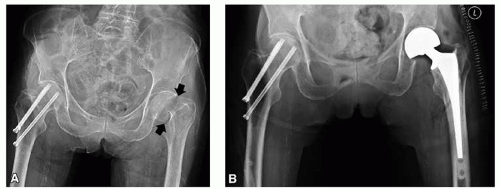 FIGURE 3-15. (A) Displaced femoral neck fracture (black arrows). (B) Treated with bipolar hemiarthroplasty. Note the prior right femoral neck fracture treated by percutaneous pinning. |
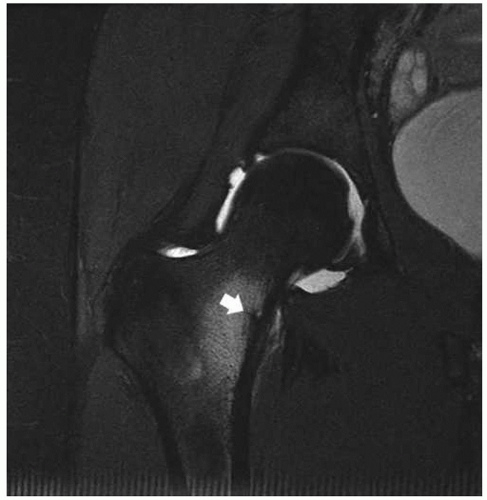 FIGURE 3-16. Femoral neck stress fracture. Coronal fast spin-echo, T2-weighted fat-suppressed image demonstrates edema with a central linear low-intensity fracture line (arrow). |
SUGGESTED READING
Berquist TH. Imaging Atlas of Orthopedic Appliances and Prostheses. New York: Raven Press; 1995:217-352.
Garden RS. Stability and union of subcapital fractures of the femur. J Bone Joint Surg. 1964;64B:630-712.
Morgan CG, Wenn RT, Sikand M, et al. Early mortality after hip fracture: is delay before surgery important. J Bone Joint Surg. 2005;87A:483-490.
Sheehan SE, Shyu JY, Weaver MJ, et al. Proximal femoral fractures: what the orthopedic surgeon wants to know Radiographics. 2015;35:1563-1584.
▪ TRAUMA: TROCHANTERIC FRACTURES
KEY FACTS
Three types of fracture: avulsion, intertrochanteric, and subtrochanteric
Intertrochanteric fractures
Most common in elderly because of falls
Extracapsular; comminution of fracture with detachment of trochanters common
Significant mortality (18% to 30%) in year of injury
Subtrochanteric fractures
More common in younger patients with high-velocity trauma
Can be associated with chronic bisphosphonate treatment
Reduction more difficult to maintain than intertrochanteric fractures
Avulsion fractures
Caused by abrupt muscle contraction (Fig. 3-17)
Occur in active athletes
Greater trochanteric avulsions also seen in elderly patients
Routine radiographs usually are diagnostic
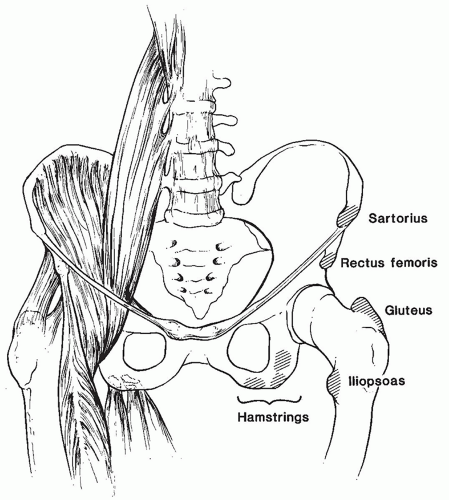 FIGURE 3-17. Sites for avulsion fractures in the pelvis and hips with muscle origins labeled. |
 FIGURE 3-18. Anteroposterior (AP) pelvic radiograph of a comminuted intertrochanteric femur fracture (black arrows) angular deformity (coxa vara deformity). |
 FIGURE 3-19. Anteroposterior (AP) hip radiograph of a subtrochanteric femur fracture with overriding and marked angulation of the fragments (coxa vara deformity). Soft tissue swelling lateral to the fracture is secondary to a hematoma. |
SUGGESTED READING
Jensen JS. Classification of trochanteric fractures. Acta Orthop Scand. 1980;51:803-810.
Lorich DG, Geller DS, Nelson JH. Osteoporotic pertrochanteric hip fractures. J Bone Joint Surg. 2004;86A:398-410.
Porrino JA Jr, Kohl CA, Taljanovic M, et al. Diagnosis of proximal femoral insufficiency fractures in patients receiving bisphosphonate therapy. Am J Roentgenol. 2010;194:1061-1064.
▪ TRAUMA: INSUFFICIENCY FRACTURES
KEY FACTS
Insufficiency fractures occur because of normal stress on bone with abnormal elastic resistance.
Insufficiency fractures most commonly involve the sacrum, pubic rami, and supra-acetabular regions and femoral necks.
Most insufficiency fractures occur in elderly osteopenic patients or patients on steroid therapy.
Patients present with back, hip, or groin pain.
Image features
Radiographs: Bone sclerosis or condensation, typically linear.
Radionuclide scans: Increased tracer in area of fracture. Bilateral sacral fractures give “H” appearance (Honda sign).
MRI: Marrow edema pattern with or without visible fracture line.
CT: Fracture lines clearly defined.
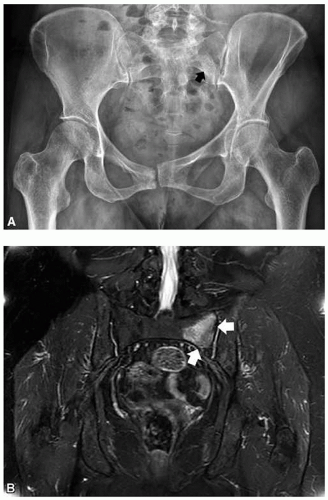 FIGURE 3-20. (A) Anteroposterior (AP) pelvis radiograph demonstrates subtle bone condensation in the left sacral ala (black arrow) caused by a sacral insufficiency fracture. (B) Coronal Short Tau Inversion Recovery (STIR) magnetic resonance (MR) image demonstrates marrow edema at the site of the fracture (white arrows). |
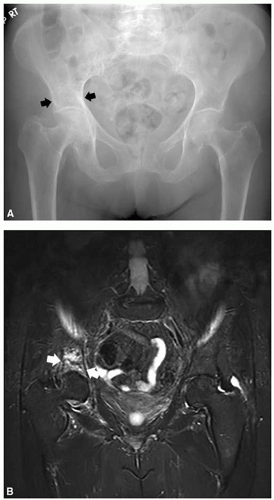 FIGURE 3-21. (A) Anteroposterior (AP) pelvis radiograph with subtle bone condensation in the right acetabulum (black arrows) caused by an acetabular insufficiency fracture. (B) Coronal STIR magnetic resonance (MR) image demonstrates a fracture line (white arrows) and adjacent marrow edema. |
SUGGESTED READING
Cabarrus MC, Ambekar A, Lu Y, et al. MRI and CT of insufficiency fractures of the pelvis and the proximal femur. Am J Roentgenol. 2008;191:995-1001.
Pek WCG, Khong PL, Yur Y, et al. Imaging of pelvic insufficiency fractures. Radiographics. 1996;16:335-348.
▪ TRAUMA: SOFT TISSUE TRAUMA
KEY FACTS
Soft tissue injuries to the pelvis, hips, and thighs may include
Muscle/tendon injuries
Ligament injuries
Neurovascular injuries
Acetabular labral tears
Bursitis
Snapping tendon syndromes
Greater trochanteric pain syndrome
Imaging approaches vary with suspected clinical condition
Condition | Imaging Approach |
Muscle/tendon injury | MRI |
Ligament injury | MRI or MR arthrography of the hip for intra-articular hip pathology |
Neurovascular injury | MRI |
Acetabular labral tears | MR arthrography of the hip |
Bursitis | Ultrasound or MRI |
Snapping tendon syndrome | Tendon injection with motion studies, ultrasound |
MR, magnetic resonance; MRI, magnetic resonance imaging. | |
SUGGESTED READING
Cvtanic O, Henzie G, Skezas DS, et al. MRI diagnosis of tears in the abductor tendons (gluteus medius and gluteus minimus). Am J Roentgenol. 2004;182:137-143.
Czermy C, Hofmann S, Nenhold A, et al. Lesions of the acetabular labrum: accuracy of MR imaging and MR arthrography in detection and staging. Radiology. 1999;220:225-230.
DeSmet AA, Fisher DR, Heiner JP, et al. Magnetic resonance imaging of muscle tears. Skeletal Radiol. 1990;19:283-286.
Khan W, Zoga AC, Meyers WC. Magnetic resonance imaging of athletic pubalgia and the sports hernia: current understanding and practice. Magn Reson Imaging Clin N Am. 2013;21:97-110.
Lonner JH, Van Kleunen JP. Spontaneous rupture of the gluteus medius and minimus tendons. Am J Orthop. 2002;31:579-581.
Rubin DA. Imaging diagnosis and prognostication of hamstring injuries. Am J Roentgenol. 2012;199:525-533.
▪ TRAUMA: SOFT TISSUE TRAUMA—MUSCLE/TENDON TEARS
KEY FACTS
Muscle/tendon tears are common in athletes and patients engaged in exercise programs.
Underlying disorders (diabetes mellitus, steroid therapy, connective tissue diseases, and renal failure) may also lead to myotendinous injuries.
Categories of injury
Grade 1 strain: a few fibers torn
Grade 2 strain: approximately 50% of fibers torn
Grade 3 strain: complete tear
Hematoma
Myositis ossificans
Muscles involved include the hamstrings, adductors, gluteal, iliopsoas, and abdominal muscles.
Radiographs or CT is useful for avulsion injuries or myositis ossificans.
MRI is superior for the detection and staging of injuries.
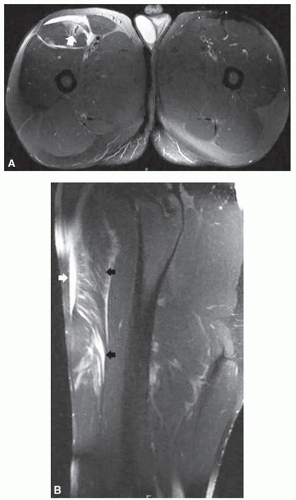 FIGURE 3-22. Axial (A) and sagittal (B) T2-weighted fat-suppressed images of a Grade 2 strain of the rectus femoris. (A) The muscle edema is centered at the myotendinous junction (white arrow). (B) Feathery edema extends through the muscle fibers (black arrows) with a small anterior hematoma (white arrow).
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|