Ankle Checklists
 1
1
Radiographic examination
AP view
Lateral view
Internal oblique view
 2
2
Common sites of injury in adults
Lateral malleolus fibula
Medial malleolus tibia
Posterior malleolus tibia
Pilon fracture of the tibial plafond
Fractures of tarsus and midfoot mimicking ankle fractures
Tarsal avulsion
Lateral view
Head of talus
Anterior cortex navicular
Posterior tuberosity of talus
Dorsal surface of calcaneal tuberosity
Anterior process of calcaneus
Tuberosity or proximal shaft of the fifth metatarsal
AP view
Lateral surface of calcaneus
Lateral process of talus
Osteochondral fractures of the dome of the talus
 3
3
Common sites of injury in children and adolescents
Epiphyseal separations of distal tibia
Salter-Harris types 1, 2, 3, and 4
Triplane fractures of distal tibia
Epiphyseal separations of distal fibula
Salter-Harris types 1 and 2
 4
4
Injuries likely to be missed
Fracture of the medial malleolus may be missed without oblique view of ankle.
Maisonneuve fracture (see
 5)
5)
Overlooked because they are not specifically sought by observer
Osteochondral fractures of the dome of the talus
Fractures of lateral process of talus
Mistake a secondary center of ossification for an avulsion or vice versa
 5
5
Where else to look when you see something obvious
| Obvious | Look for |
|---|---|
| Widening of syndesmosis | Maisonneuve fracture – associated fracture of proximal fibula |
| Widening of the medial clear space of the ankle joint | |
| Isolated fracture of posterior lip of tibia (posterior malleolus) | |
| Displaced fracture of medial malleolus without visible fracture of the distal fibula |
 6
6
Where to look when you see nothing at all
Start over again.
Check for a joint effusion and soft tissue swelling about the malleoli.
Look closely at the medial, lateral, and posterior malleoli for evidence of fracture.
Check the width of syndesmosis and medial clear space of the ankle mortise.
On the AP and oblique views look for
Osteochondral fracture at the medial and lateral corners dome of the talus
Avulsion of lateral surface of calcaneus beneath lateral malleolus
Fracture of the lateral process of talus
On the lateral view search for avulsion
Fractures of the tarsal bones of the hindfoot and midfoot (see
 2)
2)
Fracture of the tuberosity or proximal shaft of fifth metatarsal
If questionable osseous findings noted on x-ray, consider CT to evaluate further.
If x-rays are negative, consider MRI to search for occult osseous, ligament, or tendon injuries.
Ankle – The Primer
 1
1
Radiographic examination
A P view
Lateral view
Internal oblique view
Three views of the ankle are mandatory for the evaluation of the ankle following trauma. Some fractures of the medial malleolus may not be apparent on the AP and lateral views but are readily visible on the internal oblique projection.
The AP view ( Figure 11-1 A ) shows the ankle mortise; however, the lateral margin of the talus and lateral portions of the joint are obscured by the underlying lateral malleolus. Soft tissue swelling seen about the medial and lateral malleolus serves as a useful clue to the presence of an underlying acute fracture.

The internal oblique, also known as mortise view, ( Figure 11-1 B ) is obtained with 15 to 20 degrees of internal rotation of the foot. The talus and medial, lateral, and superior aspects of the joint are clearly demonstrated without significant overlap. In adults, all portions of the joint should measure 3 to 4 mm in width.
The lateral view ( Figure 11-1 C ) should include the proximal fifth metatarsal because fractures of the tuberosity often present with ankle pain and could be missed if the tuberosity were not included. On this view, the malleoli overlap, and therefore fractures at the joint line are not distinctly visualized. Joint effusions may be detected. Note the normal fat density anterior to the ankle joint on the lateral view of the normal ankle ( Figure 11-1 C ). In the presence of a joint effusion this fat is displaced by a soft tissue density that may be large enough to bulge out the overlying skin (see Figure 11-2 C ).

 2
2
Common sites of injury in adults
Lateral malleolus fibula
Medial malleolus tibia
Posterior malleolus tibia
Pilon fracture of the tibial plafond
Fractures of tarsus and midfoot mimicking ankle fractures
Tarsal avulsion
Lateral view
Head of talus
Anterior cortex navicular
Posterior tuberosity of talus
Dorsal surface of calcaneal tuberosity
Anterior process of calcaneus
Tuberosity or proximal shaft of the fifth metatarsal
AP view
Lateral surface of calcaneus
Lateral process of talus
Osteochondral fractures of the dome of the talus
Fractures of the ankle are created by movement of the talus within the ankle mortise accentuated by the leverage exerted by the foot. The principal movements are external rotation, adduction, and abduction. Secondary movements are dorsiflexion and plantar flexion. The forces are applied principally against the lateral and medial malleolus and posterior lip (posterior malleolus) of the distal tibia.
Simultaneous fractures of both the medial and lateral malleoli are described as bimalleolar fractures, whereas simultaneous fractures of all three malleoli are often referred to as trimalleolar fractures.
The bones of the ankle are bound together by intervening ligaments such as the lateral collateral and deltoid ligaments, syndesmosis, and tibiofibular ligaments. Ligaments are torn in sequence with adjacent fractures of the malleoli and distal fibula. Tensile forces in these ligaments create avulsion fractures of their bony attachments.
Viewing radiographs of the injured ankle
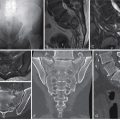
A systematic review of the injured ankle should begin with a search for soft tissue swelling (STS) about the malleoli; if present, look closely at the underlying bone for fractures ( Figures 11-2 A and 11-2 B ). Note the subtle nondisplaced transverse fracture of the lateral malleolus on both views. Ankle joint effusions present as soft tissue densities that replace the normal fat anterior to the ankle joint as seen on the lateral view ( Figure 11-2 C ). Similar densities may be seen in the pre-Achilles fat pad posterior to the joint.
Ankle fractures occur in sequence; the greater the force, the more numerous the fractures and the greater the degree of dislocations. Generally speaking, “if you see something on one side, be certain to look at the other.” That is to say, if you see a fracture of a malleolus on one side, be sure to look at the other. Then look at the posterior malleolus.
Pattern of search
Diagrams of the ankle ( Figure 11-3 ) pinpoint the common sites of fracture. The most common sites of fracture are identified by broad red lines. Less common sites are designated by fine red lines. Your pattern of search should include all sites.

Fracture of lateral malleolus
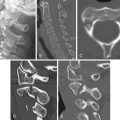
Fractures of the lateral malleolus are the most common bony ankle injuries in adults ( Figure 11-4 ). The most common injury is an oblique fracture in the coronal plane ( Figures 11-4 A and 11-4 B ). It originates anteriorly at the joint line and extends superiorly and posteriorly ( Figure 11-5 ). These fractures are due to supination-external rotation injuries. The fractures can be difficult to see on AP and oblique views when nondisplaced but are usually readily apparent on the oblique and lateral views.


Avulsions of the distal tip of the malleolus are frequent. These are the result of inversion injuries or sprains and are known as sprain fractures.
Transverse fractures at or distal to the joint line are due to adduction forces. Fractures in the oblique sagittal plane at the joint line are less common. These are due to abduction forces. Fractures located 6 to 12 cm or more above the joint line are the result of pronation-external rotation forces. The syndesmosis and interosseous membrane are always disrupted to the lowest level of the fibular fracture in such cases.
A common oblique fracture of the lateral malleolus is readily apparent in the AP view ( Figure 11-5 A ). Oblique fractures in the coronal plane are not always seen in this projection and may be better seen on the oblique view ( Figure 11-5 B ). Oblique fractures course from anterior inferior at the joint line obliquely superior and posterior as shown on the lateral view ( Figure 11-5 C ).
Other fractures of the lateral malleolus and distal fibula are shown in Figure 11-6 A . Transverse fractures and distal tip avulsions of the lateral malleolus are quite common. AP views show an avulsion at the distal tip of the lateral malleolus ( Figure 11-6 B ) and a transverse fracture of the lateral malleolus at the joint line ( Figure 11-6 C ). Oblique fractures may extend from medial at the joint line to superior and lateral in an oblique sagittal plane ( Figure 11-6 D ). More proximal fractures located between 7 and 15 cm from the joint line may present as ankle trauma ( Figure 11-6 E ). It is therefore important that all ankle radiographs include at least 16 cm of the distal tibia to avoid oversight of these more proximal injuries.