Elbow Checklists
 1
1
Radiographic examination
AP
External oblique
Lateral
 2
2
Elbow joint effusions and the fat pad sign
Visible posterior fat pad
Elevation of the anterior fat pad, the sail sign
 3
3
Common sites of injury in adults
Radial head and neck
Olecranon
Coronoid process of ulna
Distal humerus
 4
4
Common sites of injury in children and adolescents
Supracondylar of the distal humerus
Salter-Harris type 4 of lateral condyle
Avulsion of the medial epicondyle
Olecranon
 5
5
Injuries likely to be missed
Monteggia fracture dislocations
Missing radial head dislocation
Fine, subtle fractures of the radial head and neck
Radial head epiphyseal separation
 6
6
Where else to look when you see something obvious
| Obvious | Look for |
|---|---|
| Ex proximal ulna | Dislocation proximal radius |
| Fx shaft of either radius or ulna | Fx or dislocation of the other |
| Fx radial head and neck | Fx olecranon |
 7
7
Where to look when you see nothing at all
Look for joint effusion – the fat pad sign.
If present intraarticular fracture likely
In adults look at
Radial head and neck for fine fracture line
Make certain you have external oblique view.
Check tip of coronoid process for small avulsion.
In children check anterior humeral line to
Identify subtle supracondylar fracture.
Elbow – the Primer
 1
1
Radiographic examination
AP
External oblique
Lateral
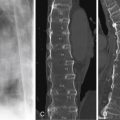
The three views ( Figure 3-1 ) selected have been proven to disclose the majority of fractures and dislocations. Certain injuries can be inapparent on standard PA ( Figure 3-1 A ) and lateral ( Figure 3-1 B ) projections and may be seen only on the external oblique view ( Figure 3-1 C ). This is particularly true of fractures of the radial head, accounting for over one-half of all fractures (60%) of the elbow in adults.

Normal elbow in children
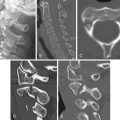
The presence and sequential appearance of multiple ossification centers in the child’s elbow ( Figures 3-2 A and B ), particularly in the distal humerus, makes for complex and potentially confusing anatomy. The capitellum is the first to appear at 3 to 5 months of age, followed by the medial epicondyle center at 4 to 6 years of age. The trochlear center appears at age 9 to 10 years. Note that the trochlear center never appears before the medial epicondylar center. The last center to appear is the lateral epicondyle at 9.4 to 11.5 years. Note the normal ossification center of the apophysis of the olecranon ( Figures 3-2 C ). This center is multipartite, a normal variant.

 2
2
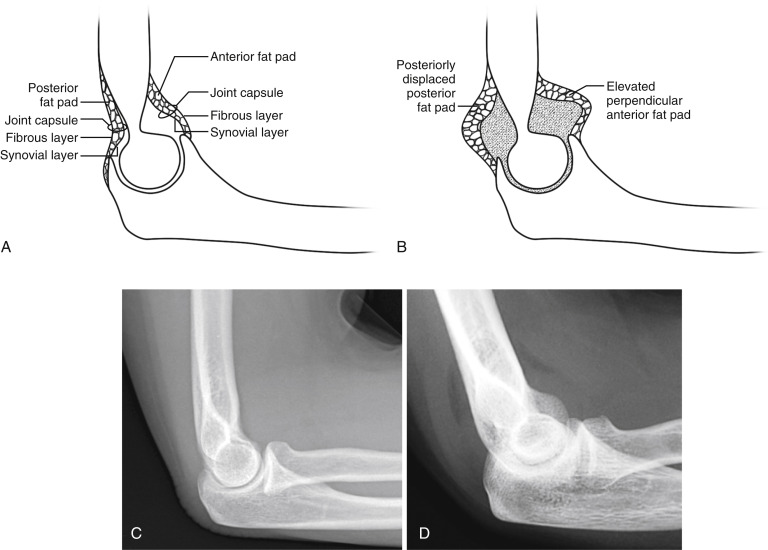
Elbow joint effusions and the fat pad sign
Visible posterior fat pad
Elevation of the anterior fat pad, the sail sign
In the setting of trauma it is very likely that an intraarticular fracture is present if a joint effusion is identified. The presence of a joint effusion is an important clue to an otherwise obscure underlying fracture of the elbow in adults as well as children and adolescents.
Elbow joint effusions are detected on the lateral view ( Figure 3-3 ). The anterior and posterior fat pads reside in the joint capsule. On the lateral view of the normal elbow ( Figures 3-3 A and C ) without a joint effusion, the posterior fat pad is not apparent, while the anterior fat pad is visible but not elevated. In the presence of a joint effusion (hemarthrosis), the fat pads are displaced, and both the anterior and posterior fat pads become visible ( Figures 3-3 B and D ). This is known as the “fat pad sign.” The posterior fat pad is displaced posteriorly, and the anterior fat pad is elevated, often referred to as the “sail sign.” Note the subtle fracture of the radial head ( Figure 3-3 D ).
 3
3
Common sites of injury in adults
Radial head and neck
Olecranon
Coronoid process of ulna
Distal humerus
Pattern of search
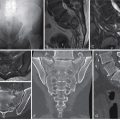
Diagrams of the elbow ( Figures 3-4 A and B ) pinpoint the common sites of fracture in adults. The most common sites of fracture are identified by broad red lines. Less common sites are designated by fine red lines. Your pattern of search should include all sites.

Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


