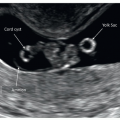
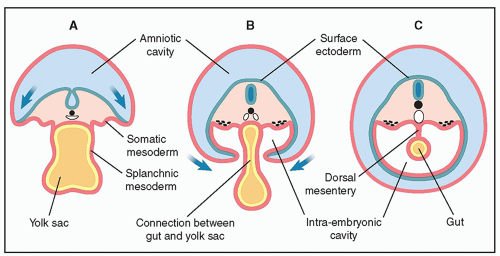
 Figure 12.1: Axial views (A-C) of the developing embryo from the fourth week of gestation showing the formation of the primitive gut tube. Note the incorporation of part of the yolk sac into the embryo, shown in A and B and the primitive gut tube “gut” shown in C. See text for details. |
ileum, cecum, ascending colon, and proximal two-thirds of transverse colon. The hindgut, supplied by the inferior mesenteric artery, gives rise to the distal one-third of transverse colon, descending colon, sigmoid, rectum, and urogenital sinus. Because of lengthening of the gut and enlargement of upper abdominal organs, an intestinal loop from the midgut protrudes through the umbilical cord insertion into the abdomen at about the sixth week of embryogenesis (from fertilization). This intestinal loop returns to the intraabdominal cavity by about the 10th week of embryogenesis (from fertilization). Through the embryologic process, the midgut loop undergoes a series of three 90-degree counterclockwise rotations around the superior mesenteric artery.
 Figure 12.2: Schematic drawing of a sagittal view of the embryo at approximately 5 to 6 menstrual weeks showing the formation of the primitive gastrointestinal tract (foregut, midgut, and hindgut) and the liver bud. Note the connection of the midgut to the vitelline duct. See text for details. |
 Figure 12.3: Axial planes at the level of the upper abdomen in two fetuses at 13 weeks of gestation. The fetus in A was examined transabdominally and the fetus in B transvaginally. Note the presence of fluid-filled stomachs (asterisks) in the upper left abdomen in A and B. Ribs (arrows) are visualized bilaterally along with the liver and inferior vena cava (IVC) in the right (R) abdomen. The descending aorta (DAo) is seen posterior and to the left of the IVC. Improved resolution is noted in fetus in B because of the transvaginal approach, thus allowing clear depiction of the IVC and DAo. L, left. |
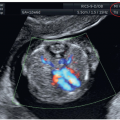
 Figure 12.4: Axial plane of the middle abdomen in gray scale (A) and color Doppler (B) at the level of the umbilical cord attachment (arrow) in a fetus at 12 weeks of gestation. Note the presence of an intact anterior abdominal wall (arrow) and the fetal bowel appearing slightly more hyperechoic than surrounding tissue. Both kidneys (K) are seen in the posterior abdomen in A. |
 Figure 12.5: Axial views of the fetal abdomen in gray scale (A) and color Doppler (B) of a fetus at 10 weeks of gestation demonstrating the presence of a physiologic midgut herniation (arrow). In the corresponding 3D ultrasound in surface mode (C), the midgut herniation is shown as a bulge at the site of cord insertion into the abdomen (arrow). |
 Figure 12.6: Axial oblique plane of the lower abdomen at 13 weeks of gestation in gray scale (A) and color Doppler (B) demonstrating the fluid-filled urinary bladder (asterisk), surrounded by the left and right umbilical arteries (UA). This view is best visualized with color Doppler (B), which can also confirm the intact abdominal wall (arrow). Note the posterior location of the iliac crests in B. |
 Figure 12.7: Parasagittal plane in two fetuses at 13 (A) and 12 (B) weeks of gestation demonstrating the thorax and abdomen. The filled stomach (asterisk) is seen under the diaphragm (arrows). Fetus A is presenting in a dorso-posterior position and fetus B in a dorso-anterior position. Note the hyperechoic lungs and bowel, the hypoechoic liver, and anechoic stomach and bladder (not shown). |
 Figure 12.8: Midsagittal view of a fetus at 13 weeks of gestation in color Doppler demonstrating the cord arising from the abdomen (arrow) with the umbilical artery (UA) and vein (UV). Ao, descending aorta. |
 Figure 12.9: Schematic drawing (A) and corresponding 3D ultrasound image in surface mode of a fetus at 12 weeks of gestation. Note the normal insertion of the umbilical cord in the abdomen in A and B (arrows). |
multiplanar display, with reconstruction of planes for the specific evaluation of target anatomic regions displayed in tomographic view of axial (Fig. 12.10) or coronal (Fig. 12.11) planes. For more details on the use of 3D ultrasound in the first trimester, refer to Chapter 3 in this book and a recent book on the clinical use of 3D in prenatal medicine.4 Figures 12.5C and 12.9 show surface mode of the fetal anterior abdominal wall and Figures 12.10 and 12.11 show the use of multiplanar mode with plane reconstruction of axial and coronal views. In our experience, multiplanar mode can be of help especially in the transvaginal approach where transducer manipulation is limited (Figs. 12.10 and 12.11).
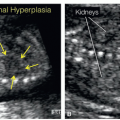
 Figure 12.10: Tomographic axial views of the abdomen in a fetus at 12 weeks of gestation showing the upper, mid, and lower abdomen. Note the presence of the stomach (asterisk) and liver in the upper abdomen, kidneys (Kid.) and abdominal cord insertion (arrow) in the mid-abdomen, and the urinary bladder (Bl.) in the lower abdomen. L, left. |
 Figure 12.11: Tomographic coronal views of the fetal chest and abdomen at 13 weeks of gestation. In this view, the diaphragm, liver, stomach (asterisk), bowel, kidneys, and urinary bladder can be seen. Note that the bowel appears echogenic because of the transvaginal approach. |
Table 12.1 • First Trimester Ultrasound and Ventral Wall Defects | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
additional anomalies of the heart, brain, kidneys, and spine. On occasion, the omphalocele can be as large or even larger than the abdominal circumference (Fig. 12.15). Follow-up of a first trimester isolated small omphalocele with a normal karyotype and nuchal translucency into the late second trimester is important because resolution of such cases has been documented in about 58% of fetuses.7 The presence of the liver in the omphalocele precludes resolution.
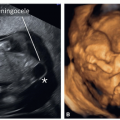
 Figure 12.12: Schematic drawing (A) and corresponding 3D ultrasound image in surface mode of a fetus at 12 weeks of gestation with an omphalocele (arrows). Note in A the presence of an omphalocele sac covering the protruding intraabdominal organs (bowel, with or without liver), with the umbilical cord attached to the top of the omphalocele. The umbilical cord is not seen in B, as the lower extremities obscure it. |
 Figure 12.13: Midline sagittal plane in two fetuses with small (A) and large (B) omphalocele (arrows) at 12 weeks of gestation. In fetus A, the omphalocele is small and contains bowel only, whereas in fetus B, the omphalocele is relatively large and contains liver and bowel. Note the presence of an enlarged nuchal translucency (asterisk) in fetus A and workup revealed trisomy 18 in this fetus. |
 Figure 12.14: Parasagittal (A) and axial (B) view of a fetus at 12 weeks of gestation with a large omphalocele (arrows). Note the presence of liver and bowel within the omphalocele. |
 Figure 12.15: Axial view of the abdominal wall at the level of the cord insertion in two fetuses at 12 (A) and 13 (B) weeks of gestation. Note the presence of a large omphalocele (asterisks) with liver and bowel content in both fetuses. In fetus A the stomach is partly in the omphalocele, whereas in fetus B the stomach has completely protruded into the omphalocele. Sp, spine. |
 Figure 12.16: Axial view of the abdominal wall at the level of the cord insertion in two fetuses at 12 (A) and 13 (B) weeks of gestation. Note the presence of a small omphalocele (arrows) in fetus A and B, with only bowel content. Trisomy 18 was diagnosed in both fetuses. |
 Figure 12.17: Sagittal (A) and axial (B) planes of the mid-abdomen in color Doppler in a fetus at 12 weeks of gestation with trisomy 18. Note the presence of a small omphalocele (asterisk) in A and B and a thickened nuchal translucency (double headed arrow) in A. The use of color Doppler is helpful because it shows the umbilical cord arising from the top of the omphalocele in A (arrow) (compare with Fig. 12.12A) and a single umbilical artery in B (arrow). |
gastroschisis is rarely associated with chromosomal or structural abnormalities. There has been an increase in the prevalence of gastroschisis worldwide.13
 Figure 12.18: Fetus with Beckwith-Wiedemann syndrome. At 13 weeks of gestation a small omphalocele with bowel content was detected, as shown in a midsagittal plane of the fetus in A. In addition, free β human chorionic gonadotropin (hCG) and pregnancy-associated plasma protein-A were elevated. Chorionic villous sampling revealed a normal karyotype. At 22 weeks of gestation, no omphalocele was found but macroglossia was noted as shown in a midsagittal and coronal planes of the face in B (arrows). The placenta also appeared thickened at 22 weeks of gestation, suggesting mesenchymal dysplasia (C). Sonographic signs were suggestive of Beckwith-Wiedemann syndrome, which was confirmed postnatally with molecular genetics. |
 Figure 12.19: Schematic drawing (A) and corresponding 3D ultrasound image in surface mode of a fetus at 13 weeks of gestation with gastroschisis. Note in A and B the presence of bowel loops anterior to the abdominal wall (arrows). There is no covering sac around the bowel and the surface of herniated bowel appears irregular.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|