the walls of the aortic vestibule, which is the septo-aortic and mitral-aortic continuity.1 For more details on cardiac embryogenesis, we recommend monographs and review articles on this subject.1, 2, 3, 4
 Figure 11.1: Frontal views of the different stages of the developing heart: in A the primitive heart tube stage, in B cardiac looping stage and in C view of the looped heart during septation of atria, ventricles and great vessels. A: Two transitional zones are identifiable: the atrioventricular ring (AVR) forming the future atrioventricular valves and the primary fold (PF) forming the future interventricular septum. B: The cardiac tube starts to loop with folding along the long axis and rotation to the right and ventral, resulting in a D-looped heart. Primitive cardiac chambers are better identified and are separated by transitional zones as the sinoatrial ring (SAR), the AVR, and the PF. C: After looping, several transitional zones can be identified separating the primitive cardiac chambers, the AVR between the common atrium (blue) and common ventricle (red), the PF between the primitive left (LV) and right (RV) ventricle, and the VAR in the conotruncus (CT) region of the outflow tract of the heart. RA, right atrium; LA, left atrium. |
can be obtained in the first trimester under optimal scanning conditions. Based upon our experience however, visualization in the first trimester of four essential planes—(1) the axial view of the upper abdomen, (2) the 4CV in gray scale, (3) the 4CV in color Doppler, and (4) the 3VT in color Doppler (Fig. 11.5)—provides enough information to rule out most major cardiac malformations.
 Figure 11.2: Typical planes displayed in gray scale during the first trimester cardiac examination include the visualization of the abdominal situs (A) with stomach (asterisk) and the four-chamber view, displayed in a transverse (B) or in an apical view (C). LV, left ventricle; RV, right ventricle; R, right; L, Left. |
Table 11.1 • Optimization of the gray-scale cardiac examination in the first trimester | ||||||||
|---|---|---|---|---|---|---|---|---|
|
Table 11.2 • Optimization of Color Doppler Cardiac Examination in the First Trimester | ||||||||
|---|---|---|---|---|---|---|---|---|
|
 Figure 11.3: Color Doppler of an apical four-chamber view at 12 weeks of gestation by transabdominal (A) and transvaginal (B) ultrasound examination demonstrating diastolic flow from both right (RA) and left (LA) atrium into right (RV) and left (LV) ventricle, respectively. Note that the heart in B is displayed with a higher resolution due to the transvaginal approach. |
 Figure 11.4: Transvaginal ultrasound of the outflow tracts in color Doppler in a fetus at 13 weeks of gestation showing the five-chamber view (A), the short axis view of the right ventricle (RV) (B), and the three-vessel-trachea view (C). Ao, aorta; LV, left ventricle; PA, pulmonary artery; SVC, superior vena cava. |
 Figure 11.5: Four essential planes in the first trimester cardiac examination include the plane at the abdominal circumference level (A) to visualize abdominal situs with the stomach (asterisk) on the left side, the four-chamber view (B) in gray scale, as well as the four-chamber view in color Doppler in diastole (C) and the three-vessel-trachea view in color Doppler in systole (D). LV, left ventricle; RV, right ventricle; PA, pulmonary artery; Ao, aorta; R, right; L, Left. |
in early gestation. Figure 11.6 shows a fetus at 13 weeks of gestation with deletion 22q11.2 detected with targeted FISH performed due to the presence of polydactyly and an interrupted aortic arch seen on the first trimester ultrasound.
 Figure 11.6: Fetus at 13 weeks of gestation with deletion 22q11. Note in A the presence of a normal facial profile with normal nuchal translucency (NT). Also note in A the presence of hexadactyly (numbers 1-6), shown in hand. In B, the four-chamber view demonstrates a ventricular septal defect (VSD). C: Obtained at the three-vessel-trachea view and shows an interrupted aortic arch (IAA) (arrows). Chorionic villous sampling with targeted FISH confirmed the suspected deletion 22q11. AAO, ascending aorta; DA, ductus arteriosus; LV, left ventricle; PA, pulmonary artery; RV, right ventricle. |
Table 11.3 • Suggested Indications for Fetal Cardiac Imaging in the First Trimester | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
an absent or reversed A-wave during the atrial contraction phase of diastole (Fig. 11.8A). This flow pattern in the first trimester has been associated with an increased risk of aneuploidy. In chromosomally normal fetuses, abnormal DV waveforms have also been shown to be associated with structural cardiac anomalies.17 The underlying pathophysiologic mechanism linking the reversed DV A-wave to fetal CHD is unclear, but an increased right atrial preload as a result of an increase in volume, pressure, or both in CHD could be one of the underlying mechanisms. Detecting a reversed A-wave in the DV increases the risk for the presence of CHD in the fetus.16
 Figure 11.7: Relationship between increased nuchal translucency (NT) thickness and risk of congenital heart disease (CHD) based on a meta-analysis of 12 studies. Note that the prevalence of CHD increases with increased NT thickness. (Adapted from Clur SA, Ottenkamp J, Bilardo CM. The nuchal translucency and the fetal heart: a literature review. Prenat Diagn. 2009;29:739-748; copyright John Wiley & Sons, Ltd., with permission.) |
 Figure 11.8: A: Pulsed Doppler of ductus venosus (DV) in a fetus at 13 weeks of gestation with a cardiac defect, showing reversed flow in the A-waves (open circle) during atrial contractions. The presence of this pattern suggests an increased risk for associated cardiac abnormalities. B: Pulsed Doppler of the tricuspid valve (long arrow) in a fetus with a tetralogy of Fallot. Note the presence of tricuspid regurgitation on pulsed Doppler (opposing arrows). The presence of tricuspid regurgitation increases the risk for the presence of cardiac abnormalities. S, peak systolic velocity; D, peak diastolic velocity. |
 Figure 11.9: Cardiac axis (blue arrows) measurement in two fetuses at 13 weeks of gestation in color Doppler. In fetus A with a normal heart anatomy, the cardiac axis is normal. In fetus B with an atrioventricular septal defect (AVSD) and ventricle disproportion with aortic coarctation (CoA), the cardiac axis is deviated with a wide angle. Cardiac axis is measured in a four-chamber view of the heart by the angle of two lines; the first line starts at the spine (S) posteriorly and ends in mid-chest anteriorly, bisecting the chest into two equal halves, the second line runs through the ventricular septum. RV, right ventricle; LV, left ventricle; L, left. |
reverse flow on color Doppler (Figs. 11.11C and 11.12C). An echogenic globular left ventricle can occasionally be seen in the first trimester in HLHS (Fig. 11.13) and represents left ventricular changes (fibroelastosis), similar to that noted in the second and third trimesters of pregnancy. Of note is that the presence of a “normal” four-chamber view in the first trimester cannot rule out HLHS, as it has been shown to develop between the first and second trimesters of gestation.
Table 11.4 • Abnormal Ultrasound Findings and Suspected Cardiac Anomalies in the First Trimester | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||
 Figure 11.10: Schematic drawings of hypoplastic left heart syndrome (HLHS). Note in A the typical features of hypoplastic hypokinetic left ventricle (LV), dysplastic mitral valve, atretic aortic valve, and hypoplastic aorta (Ao). B: The infrequent type of HLHS in the first trimester with dilated, hyperechogenic left ventricle (fibroelastosis), narrowing at the aortic valve level and obstruction to left ventricular outflow, in association with critical aortic stenosis. RA, right atrium; RV, right ventricle; PA, pulmonary artery; LA, left atrium. |
associated genetic syndromes, such as Turner syndrome, Noonan syndrome, Smith-Lemli-Opitz syndrome, and Holt-Oram syndrome.21 Fetuses with HLHS may develop growth restriction in the late second and third trimesters of pregnancy probably due to a 20% reduction in combined cardiac output.22 When HLHS is diagnosed in the first trimester, follow-up ultrasound examinations are recommended.
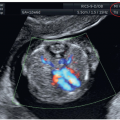
 Figure 11.11: Hypoplastic left heart syndrome in a fetus at 13 weeks of gestation demonstrated by transabdominal ultrasound. Note in A the absence of a left ventricle (arrow) in the four-chamber view. In B, color Doppler shows diastolic flow between right atrium (RA) and right ventricle (RV) with absent left ventricular flow. In C, three-vessel-trachea view in color Doppler shows antegrade flow in the pulmonary artery (PA) (blue arrow) and retrograde flow into the aortic arch (AoA) (red arrow). LA, left atrium. |
 Figure 11.12: Hypoplastic left heart syndrome in a fetus at 13 weeks of gestation demonstrated by transvaginal ultrasound (different fetus than in Fig. 11.11). Note in A the absence of a left ventricle (LV) in the four-chamber view. In B, color Doppler shows diastolic flow between right atrium (RA) and right ventricle (RV) with absent left ventricular flow. In C, three-vessel-trachea view in color Doppler shows antegrade flow in the pulmonary artery (PA) and retrograde flow into the small aortic arch (AoA). Note the increased resolution in the ultrasound images as compared to Figure 11.11 obtained transabdominally. Compare with Figure 11.11. LA, left atrium. |
 Figure 11.13: Four-chamber view in a fetus with hypoplastic left heart syndrome (HLHS) at 13 weeks of gestation with gray-scale (A) and color Doppler (B) imaging. Note the presence in A of a relatively small echogenic left ventricular (LV) cavity. Color Doppler in B shows absence of mitral inflow during diastole. The presence of an echogenic LV is unusually found in HLHS in the first trimester in comparison with the second trimester. RA, right atrium; RV, right ventricle; LA, left atrium.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|