Foot Checklists
 1
1
Radiographic examination
AP
Oblique
Lateral
Axial view of calcaneus
 2
2
Common sites of injury in adults
Metatarsals
Neck, base, shaft
Fifth MT – tuberosity, Jones’ fracture
Phalanges
Metatarsal/tarsal fracture-dislocation (Lisfranc)
Calcaneus – compression fracture
Talus
Neck
Lateral process (snowboarder’s fracture)
Subtalar fracture-dislocation
Chopart’s fracture-dislocation
Navicular
Body
Proximal pole
Tarsal avulsion
Lateral view
Head of talus
Anterior cortex navicular
Posterior tuberosity of talus
Dorsal surface of calcaneal tuberosity
Anterior process of calcaneus
AP view
Lateral surface of calcaneus
 3
3
Common sites of injury in children and adolescents
Metatarsal
Bunk bed fracture (buckle fracture base of first MT)
Apophysis base of fifth MT (do not mistake for fracture)
Phalanges
Salter-Harris types 1 and 2 epiphyseal separation
Calcaneus
Under age 14 – extra articular fx of tuberosity
Over age 14 – adult pattern intraarticular compression fx
Talus
Nondisplaced fx of neck of talus; may be torus or buckle-type fx
 4
4
Injuries likely to be missed
Minimally displaced Lisfranc fracture-dislocations
Fracture of adjacent metatarsals
Lateral process fractures of talus (snowboarder’s fx)
Subtle nondisplaced fractures of base of metatarsals
 5
5
Where else to look when you see something obvious
| Obvious | Look for |
|---|---|
| Fx metatarsal | Fxs adjacent metatarsals |
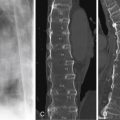
| Compression fx calcaneus | Similar fx opposite calcaneus |
| Compression fx thoracolumbar spine |
 6
6
Where to look when you see nothing at all
Lisfranc fracture-dislocation
Fine nondisplaced fracture of the neck of the talus
Fine nondisplaced fracture of anterior process of calcaneus
Subtle fine fracture of neck or base of metatarsals
If questionable radiographic findings – CT to clarify abnormality
If radiographs negative – MRI to identify ligament tears, tendon injuries, and bone contusions
Foot – The Primer
 1
1
Radiographic examination
AP
Oblique
Lateral
Axial view of calcaneus
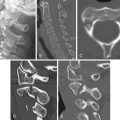
A minimum of three views—AP ( Figure 12-1 A ), internal oblique ( Figure 12-1 B ) and lateral ( Figure 12-1 C )—should be obtained. In some cases fractures of the phalanges are seen only on the internal oblique view and, therefore, may be overlooked if the internal oblique is omitted. If there is a question of injury to the calcaneus, an axial view of the calcaneus ( Figures 12-1 D and 12-1 E ) should be obtained in addition to the standard views of the foot. When the suspected injury is confined to the toes, AP ( Figure 12-1 F ), oblique, and lateral views of the toes should be obtained rather than the foot, as detail is increased and disclosure of injuries is enhanced.

 2
2
Common sites of injury in adults
Metatarsals
Neck, base, shaft
Fifth MT – tuberosity, Jones’ fracture
Phalanges
Calcaneus
Compression fracture
Noncompressive fractures
Avulsion
Anterior process
Beak fracture tuberosity
Lateral body (extensor digitorum brevis avulsion)
Talus
Neck
Lateral process (snowboarder’s)
Posterior tuberosity
Navicular
Body
Proximal pole
Anterior-superior cortical avulsion
Dislocation
Metatarsal/tarsal fracture-dislocation (Lisfranc)
Subtalar fracture-dislocation
Chopart’s fracture-dislocation
Pattern of search in adults
AP and lateral diagrams of the foot ( Figure 12-2 ) pinpoint the common sites of fracture. The most common sites of fracture are identified by broad red lines. Less common sites are designated by fine red lines. Your pattern of search should include all sites.

Metatarsal and phalangeal fractures account for the majority of fractures of the foot. Metatarsal fractures are frequently multiple, with similar fractures involving the same site: neck ( Figure 12-3 A ), shaft, or base ( Figure 12-3 B ) of adjacent metacarpals. Having identified one metatarsal fracture, look closely at adjacent metatarsals for similar fractures. Similar fractures of adjacent phalanges are less common.

Fractures of the fifth metatarsal are quite common. Avulsions of the tuberosity ( Figure 12-4 A ) should be distinguished from fractures of the base or the shaft of the metatarsal (also known as Jones’ fracture) ( Figure 12-4 B ).

Fractures of the phalanges are often due to heavy objects falling on the foot ( Figure 12-5 A ) or stubbing the toe while walking barefoot ( Figure 12-5 B ). Mach bands formed by the underlying sole of the foot or overlapping toes ( Figure 12-5 C ) should not be mistaken for fractures. It is imperative that oblique views of the toes be obtained to avoid missing fractures, as some fractures of the phalanges may only be visualized on the oblique projection ( Figures 12-6 A and 12-6 B ). Dislocations of the metatarsophalangeal and interphalangeal joints are common ( Figure 12-7 A ). Make certain the joint is properly aligned on the postreduction radiograph. Note the slight malalignment of the third PIP joint on the postreduction examination ( Figure 12-7 B ). This malalignment proved to be due to entrapment of a flexor tendon.



Calcaneus
Fractures of the calcaneus are divided into two types, noncompressive and compression.
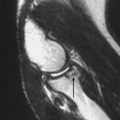
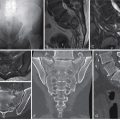
Noncompressive are avulsions of the periphery of the bone: extensor digitorum brevis avulsion from the lateral aspect of the body as seen on AP views of the ankle beneath the lateral malleolus, posterior superior tuberosity (beak fracture) ( Figure 12-8 A ), and anterior process avulsion (arrow) ( Figure 12-8 B ). An anterior process avulsion should be differentiated from a secondary center of ossification, the os calcaneus secondarius (arrow) ( Figure 12-8 C ).

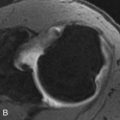
Compression fractures are due to high-impact trauma either falls from great heights and landing on the feet or in motor vehicle crashes. In compression fractures the posterior facet is fractured and compressed into the body of the calcaneus ( Figure 12-9 A ).