Hand Checklists
 1
1
Radiographic examination
PA
Pronation oblique
Lateral
 2
2
Common sites of injury in adults
Fractures
Phalanges (55% of hand injuries)
Distal (50+% of fractures of the phalanx)
Ungual tuft, base, shaft, baseball finger avulsion
Proximal (15% of fractures of the phalanx)
Shaft, base, condyles, volar plate avulsion
Middle (10+% of fractures of the phalanx)
Shaft, base, condyles, volar plate avulsion
Metacarpals (36% of hand injuries)
Shaft, base, head, neck (boxer’s fracture of fourth and fifth MCs)
Thumb
Base of metacarpal
Intraarticular – Bennett’s, Rolando’s
Extraarticular – transverse, oblique
Distal phalanx
Ungual tuft, base, shaft
Dislocations
Interphalangeal joints (DIP and PIP)
Metacarpophalangeal joints
Carpometacarpal joints
Fourth and fifth CMC fracture dislocation most common
 3
3
Common sites of injury in children and adolescents
50% involve the proximal phalanx.
Majority of fractures of the phalanges and metacarpals
- a.
involve the epiphysis
- b.
Salter-Harris type 2, most common
- a.
High percentage best seen on the oblique view.
 4
4
Injuries likely to be missed
Fracture-dislocations of the fourth and fifth carpometacarpal (CMC) joints
Fractures of the condyles of the phalanges
 5
5
Where else to look when you see something obvious
Fractures of adjacent metacarpals and phalanges
Fractures base of fourth and fifth MCs – dislocation of adjacent MCC joint
 6
6
Where to look when you see nothing at all
Start over again – review the radiographs.
Consider
CT for questionable radiographic findings
MRI if radiographs are unrevealing
Hand – The Primer
 1
1
Radiographic examination
PA
Pronation oblique
Lateral
The standard radiographic examination of the traumatized hand should include the three standard views: PA ( Figure 5-1 A ), pronation oblique ( Figure 5-1 B ), and lateral ( Figure 5-1 C ). Many fractures are more apparent and better visualized on the oblique projection. Fractures may be missed if the examination is limited to only the PA and lateral projections. For the lateral view ( Figure 5-1 C ) the fingers should be “fanned” to allow clear visualization of each finger without overlap of the digits.

When the injury is confined to a single digit, a phalanx, greater detail and a sharper image are obtained by limiting the exposure to the digit in question as shown in Figure 5-2 of left index finger: PA view, ( Figure 5-2 A ), oblique view ( Figure 5-2 B ), and lateral view ( Figure 5-2 C ). This is particularly useful in identifying volar plate avulsions and other fine nondisplaced fractures that can be quite subtle and can be overlooked on radiographs of the entire hand. The same may be said of the thumb as shown in Figure 5-3 of the right thumb: PA view ( Figure 5-3 A ), oblique view ( Figure 5-3 B ), and lateral view ( Figure 5-3 C ).


 2
2
Common sites of injury in adults
Fractures
Phalanges (55% of hand injuries)
Distal (50+% of fractures of the phalanx)
Ungual tuft, base, shaft, baseball finger avulsion
Proximal (15% of fractures of the phalanx)
Shaft, base, condyles, volar plate avulsion
Middle (10+% of fractures of the phalanx)
Shaft, base, condyles, volar plate avulsion
Metacarpals (36% of hand injuries)
Shaft, base, head, neck (boxer’s fracture of fourth and fifth MCs)
Thumb
Base of metacarpal
Intraarticular – Bennett’s, Rolando’s
Extraarticular – transverse, oblique
Distal phalanx
Ungual tuft, base, shaft
Dislocations
Interphalangeal joints (DIP and PIP)
Metacarpophalangeal joints
Carpometacarpal joints
Fourth and fifth CMC fracture dislocation most common
Pattern of search
Diagrams of the hand pinpoint the common sites of fracture and dislocation in adults ( Figures 5-4 A , PA view, and 5-4 B , lateral view). The most common sites are identified by thicker red lines. Less common sites are designated by fine red lines. Your pattern of search should include all sites.

Fractures of the hand are undoubtedly the most common sites of fracture in the entire skeleton. Fractures of the phalanges account for over 55%, most frequently involving the distal phalanx. Slightly fewer than 40% of fractures involve the metacarpals, most commonly the fifth metacarpal followed by the thumb metacarpal.
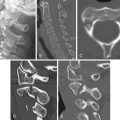
Soft tissue swelling serves as a clue to fractures of the phalanges. When encountered look closely at the underlying bone and joints for subtle injuries ( Figure 5-5 A , PA view, note swelling about PIP joint and head of proximal phalanx; Figure 5-5 B , lateral view, note avulsion of volar surface of epiphysis of middle phalanx better seen on Figure 5-5 C ).

Fractures of the ungual tuft ( Figure 5-6 A ) are one of the most common fractures in the hand and are best seen when examination is limited to the digit in question. They are easily overlooked on radiographs of the hand either because the distal tips of the fingers are overexposed or in the absence of clinical information directing attention to them. Always look specifically at the ungual tufts for evidence of fracture. Longitudinal fractures may occur ( Figure 5-6 B ). A fine, nondisplaced, intraarticular Y-shaped fracture of the base of the distal phalanx is shown in Figure 5-6 C .

Small avulsions occur from volar surface of the base of the middle phalanx ( Figure 5-7 A ) and, less commonly, of the distal phalanx. These are due to hyperextension injuries and represent avulsions at the attachment of the volar plate and are therefore referred to as volar plate avulsions. Avulsion fractures also occur from the dorsal surface of the base of the terminal phalanx ( Figure 5-7 B ) often associated with a flexion deformity of the DIP. The fracture is created by pull of the extensor tendon that inserts on the dorsal surface of the base of the terminal phalanx. These usually occur in ballplayers when the ball hits the end of the finger and are therefore known as baseball fingers. The injury is also referred to as a mallet finger because flexion deformities of the DIP suggest the appearance of a hammer.

Fractures of the shafts of the phalanges may be transverse or oblique ( Figure 5-8 A ). Fractures of the base of the proximal phalanx are characteristically sharply angulated dorsally ( Figure 5-8 B ). Fractures of the condyle ( Figure 5-8 C ) require open reduction and pin or screw fixation. Pathologic fractures occurring in the phalanges virtually all involve benign enchondromas ( Figure 5-8 D ).

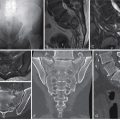
Boxer’s fractures occur at the neck of the fourth and fifth MCs ( Figure 5-9 A ). These are the result of a blow struck by the fist. The distal fragment is usually in volar angulation. Oblique fractures occur in the midshaft ( Figure 5-9 B ) and may be obscure when nondisplaced. Transverse fractures are common ( Figures 5-9 C and 5-9 D ). Fractures of the base of the metacarpals, particularly the fourth and fifth metacarpals) are often accompanied by dislocation of the adjacent carpometacarpal joint ( Figure 5-9 E ).

Fractures of the thumb
Fractures of the thumb most frequently involve either the terminal phalanx or the base of the thumb. Terminal phalanx fractures are similar to those of the other phalanges. Fractures of the base of the metacarpal ( Figure 5-10 A ) are either intraarticular Bennett’s fracture dislocations ( Figure 5-10 B ), comminuted Rolando’s fractures, or extraarticular transverse ( Figure 5-10 C ) or oblique fractures that spare the carpometacarpal joint.

Dislocations of the phalanges
Dislocations are common in both the PIP ( Figure 5-11 A ), DIP, and MCP ( Figure 5-11 B ) joints and are frequently accompanied by fractures of the base of the displaced phalanx. Carpometacarpal dislocations are less common but may be subtle, difficult to identify, and easily overlooked, particularly those involving the fourth and fifth MCs ( Figures 5-11 C and 5-11 D ). To avoid oversights, be certain to look specifically for evidence of fourth and fifth CMC fracture dislocations in every case. Note fracture of the base of the fourth MC and obliteration of the fifth MCC joint space due to dislocation of the fifth MCC joint ( Figure 5-11 C ). Note malalignment of MCs and small avulsion fracture from the dorsal surface of the distal hamate on the lateral view ( Figure 5-11 D ).