44
The Tree-in-Bud Pattern
One characteristic feature of bronchiolar disease is a tree-in-bud pattern on computed tomography (CT); the other is centrilobular nodules. The tree-in-bud pattern was first used as a descriptor by Im et al. to describe the appearance of the endobronchial spread of mycobacterial tuberculosis. This pattern is manifested by luminal filling of contiguous branching segments of bronchioles seen in bronchiolar disease. Bronchiolitis and bronchiolectasis are nonspecific inflammatory processes (sometimes associated with fibrotic bronchiolitis) of the small airways caused by many different conditions. Imaging of bronchiolar disease is best performed by thin-section CT.
Bronchiolar Anatomy
Bronchioles, small airways with an internal diameter of <2 mm, do not contain cartilage in their walls, consist of membranous or terminal bronchioles that are purely air conducting, and respiratory bronchioles containing alveoli in their walls, distal to the 7th or 8th generation of the tracheobronchial tree. The secondary pulmonary lobule, measures 10 to 25 mm in diameter, is the smallest portion of the lung that is surrounded by connective tissue septa. Each lobule is supplied by a lobular bronchiole (≤1 mm in diameter) and a pulmonary artery branch, both of which are located in the center of the secondary lobule. Because visibility on CT is typically limited to bronchi >2 mm in diameter, normal lobular bronchioles cannot be seen on CT scans. However, diseased bronchioles (bronchiolar wall thickening, bronchiolar dilatation, and luminal impaction) can be visualized as a tree-in-bud pattern. This pattern is analogous to the large airway “finger-in-glove” appearance of bronchial impaction, but on a much smaller scale. Indirect signs of bronchiolar disease on CT include mosaic attenuation, air trapping, and subsegmental atelectasis especially on expiratory CT scanning.
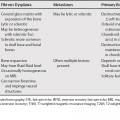
Differential Diagnosis Based on a Tree-in-Bud Pattern