Wrist Checklists
 1
1
Radiographic examination
Carpus
PA
PA with ulnar deviation
Pronation oblique
Lateral
Distal forearm
PA
Pronation oblique
Lateral
 2
2
Common sites of injury in adults
Distal radius and ulnar styloid
Scaphoid
Waist, distal tubercle, proximal pole
Triquetrum
Dorsal surface
Hamate
Dorsal and distal surface often in association with fourth and fifth MCC joint fracture-dislocation
 3
3
Common sites of injury in children and adolescents
Both bone fractures of distal forearm common
Buckle (torus) fractures may be subtle.
Distal radial epiphyseal separations, Salter-Harris types 1 and 2
Most common site of epiphyseal separations in entire skeleton
Salter-Harris type 1 in younger children
Salter-Harris type 2 most common in older children and adolescents
Carpal fractures uncommon in young children.
 4
4
Injuries likely to be missed
Fine, nondisplaced fracture of scaphoid
Waist, proximal pole, distal tubercle
Subtle, nondisplaced fracture of distal radius
Fracture-dislocation of fourth and fifth MCC joints
 5
5
Where else to look when you see something obvious
| Obvious | Look for |
|---|---|
| Fracture ulnar styloid | Subtle fracture distal radius |
| Fracture dorsal surface hamate | Dislocation fourth and fifth MCC |
| Displaced fracture scaphoid | Fracture capitate and/or triquetrum |
| Perilunate dislocation | |
| Fracture distal shaft radius | Galeazzi fracture dislocation, disrupt distal radial ulnar joint |
| Dislocation distal radioulnar joint | Comminuted fx radial head – (Essex-Lopresti fracture) |
 6
6
Where to look when you see nothing at all
Note pronator quadratus sign.
Clue to underlying subtle distal radial fracture
Look closely at scaphoid for fine fracture line.
Waist, proximal pole, distal tubercle
Check dorsal surface of triquetrum and hamate on lateral view.
Observe integrity of fourth and fifth MCC joints.
If questionable radiographic findings, get CT.
If x-rays negative but clinical concern for significant injury, get MRI.
Wrist – the Primer
 1
1
Radiographic examination
Carpus
PA
PA with ulnar deviation
Pronation oblique
Lateral
Distal forearm
PA
Pronation oblique
Lateral
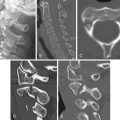
These four views ( Figures 4-1 A , PA, 4-1 B , PA with ulnar deviation, 4-1 C , pronation oblique, and 4-1 D , lateral) are selected because they have been proven to disclose the presence of the majority of fractures and dislocations.

Fractures of the waist of the scaphoid are notorious for being inapparent on the PA view ( Figure 4-1 A ); however, the PA view with ulnar deviation ( Figure 4-1 B ) will usually disclose these otherwise obscure fractures.
Certain injuries can be inapparent on standard PA and lateral orthogonal projections but become evident on the pronation oblique view ( Figure 4-1 C ). This is particularly true of subtle fracture dislocations of the fourth and fifth MCC joints, fractures of the distal tubercle of the scaphoid, and obscure, nondisplaced fractures of the distal radius.
 2
2
Common sites of injury in adults
Distal radius and ulnar styloid
Scaphoid
Waist, distal tubercle, proximal pole
Triquetrum
Dorsal surface
Hamate
Dorsal and distal surface
Commonly in association with dislocations of the fourth and fifth MCC joints
Base of the fourth and fifth metacarpals, fractures or MCC fracture-dislocations
Pattern of search
Diagrams of the wrist and distal forearm ( Figure 4-2 ) pinpoint the common sites of fracture. The most common sites of fracture are identified by broad red lines. Less common sites are designated by fine red lines. Your pattern of search should include all sites. The fourth and fifth metacarpohamate joints should be examined closely to detect fractures of the base of the metacarpals or fracture dislocations of the MCC joints. The MCC joint spaces should be of normal width, similar to the second and third MCC joints, and the opposing cortical surfaces of the fourth and fifth MCC joints should be parallel.

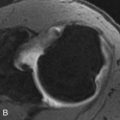
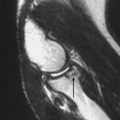
Pronator quadratus fascial plane
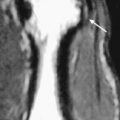
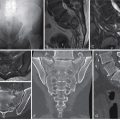
The pronator quadratus muscle extends across the volar surface of the ulna to insert on the volar and ulnar surfaces of the distal radius ( Figure 4-3 A ). The fascial surface of the muscle is outlined by a thin layer of fat that is visible on lateral radiographs of the wrist ( Figure 4-3 B ). Changes in the appearance of the pronator fascia plane are clues to otherwise obscure underlying fractures of the distal radius. Normally this fascial plane is seen on a lateral radiograph of the wrist as a linear lucent line extending proximally from the volar rim of the distal radial joint surface ( Figures 4-3 B and 4-4 A and B , small arrow). In the presence of a fracture of the distal radius, the fascial plane is bowed and displaced outward by hemorrhage and edema within the underlying pronator quadratus muscle. Note bulging pronator fascial plane due to subtle, torus-like impacted fracture of the dorsal distal radial metaphysis ( Figure 4-4 C ).

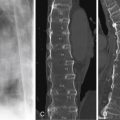
Fractures of the distal radius and ulna
Fractures of the distal radius and ulna are 10 times more frequent than fractures of the carpal bones. The majority are either nondisplaced or Colles fractures with dorsal angulation of the distal fragment ( Figures 4-4 to 4-6 A and B ). Colles fractures are ≈10 times more frequent than Smith fractures characterized by volar angulation of the distal fragment ( Figures 4-5 and 4-6 C and D ). Care should be taken to differentiate between the two.



Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


