34 Thyroid nodules are commonly encountered and are seen in up to 41 to 67% of the population on ultrasound and in up to 50% of the population on autopsy. The incidence of cancer in thyroid nodules sent for fine-needle aspiration (FNA) is 9.2 to 13%, regardless of how many nodules are present in the gland. In patients with multiple nodules, the cancer is in the nondominant nodule approximately one third of the time. Punctate, linear, eggshell, amorphous, and nodular calcifications can occur in benign and malignant thyroid tumors. Fine punctate calcifications are more characteristic of malignancy; when found within a solid nodule on ultrasound, they have been shown to predict a threefold increase in cancer risk. However, it has been reported that 38% of patients with microcalcifications had benign lesions. Calcifications have also been shown to become more prevalent as a patient ages and as the duration of multinodular goiter grows. Cysts have low T1-weighted and high T2-weighted magnetic resonance (MR) signal intensities. Cysts with high thyroglobulin concentrations are hyperintense on T1-weighted MR images (T1WI) and T2-weighted MR images (T2WI). Cysts with colloid or hemorrhage may also be hyperintense on T1WI. Hemorrhagic necrosis is prevalent in high-grade malignant tumors, especially in anaplastic carcinoma (60 to 70%), and less common in low-grade tumors. Hemorrhage may occasionally occur in a large goiter.
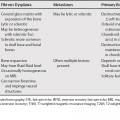
Thyroid Diseases and Lesions
Calcifications
Cysts and Hemorrhage
Cancer and Metastases
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


