Tracheal Neoplasms
Jud W. Gurney, MD, FACR
Key Facts
Terminology
Rare malignant (90%) neoplasms of chest (0.1%), 2/3 either squamous cell carcinoma or adenoid cystic carcinoma
Imaging Findings
Proximal 1/2 of trachea: Adenoid cystic carcinoma
Lower 1/3 of trachea: Squamous cell carcinoma
Usually < 2.5 cm in size (otherwise would completely occlude trachea)
Tracheal lesions often overlooked (sensitivity 25-50%) on chest radiographs
Calcification in tumor not benign finding; seen in chondrosarcoma, carcinoid, mucoepidermoid carcinoma
Top Differential Diagnoses
Wegener Granulomatosis
Amyloidosis
Relapsing Polychondritis
Pathology
Top 5 (90% of tracheal tumors): Squamous cell carcinoma, adenoid cystic carcinoma, carcinoid, squamous cell papilloma, mucoepidermoid carcinoma
Diagnostic Checklist
Consider
Tracheal tumors in any patient with shortness of breath unresponsive to bronchodilators
Tracheal tumors if patient has dyspnea at night
Synchronous or metachronous 2nd primaries common (up to 40%)
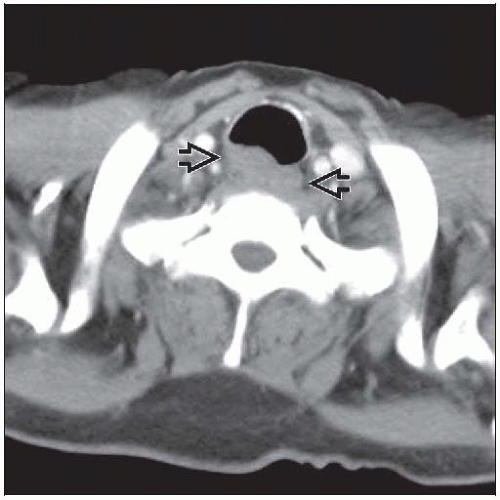 Axial CECT shows a lobulated homogeneous mass involving the posterior tracheal wall  in this patient with squamous cell carcinoma. in this patient with squamous cell carcinoma. |
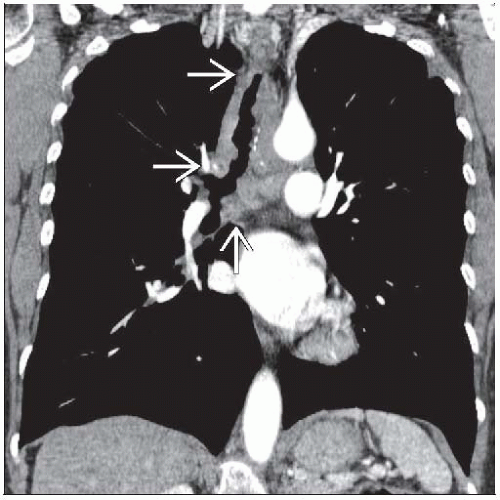 Coronal CECT shows diffuse tracheal wall thickening  in a patient with adenoid cystic carcinoma. The longitudinal extent of the tumor exceeds the axial extent. in a patient with adenoid cystic carcinoma. The longitudinal extent of the tumor exceeds the axial extent. |
TERMINOLOGY
Definitions
Rare malignant (90%) neoplasms of chest (0.1%), 2/3 either squamous cell carcinoma or adenoid cystic carcinoma
IMAGING FINDINGS
General Features
Patient position/location
Proximal 1/2 of trachea: Adenoid cystic carcinoma
Lower 1/3 of trachea: Squamous cell carcinoma
Size: Usually < 2.5 cm (otherwise would completely occlude trachea)
Imaging Recommendations
Best imaging tool: CT method of choice to characterize extent of tumor
CT Findings
General findings similar in all intratracheal tumors
Factors favoring malignancy
Extraluminal extension
Circumferential involvement
Lobulated or irregular margin
Contrast enhancement with intravenous contrast
Factors favoring benignancy
Sessile or polypoid
Intraluminal only
Smooth and sharply marginated
Squamous cell carcinoma and adenoid cystic carcinoma have similar features, helpful distinguishing features
Squamous cell may be multifocal (10%)
Squamous cell more common to have regional lymph node enlargement
Adenoid cystic longitudinal extent > transaxial extent and tumor usually more than 180° of airway circumference
Fat content suggests lipoma or hamartoma
Calcification in tumor not benign finding; seen with chondrosarcoma, carcinoid, mucoepidermoid carcinoma
Radiographic Findings
Radiography
Tracheal lesions often overlooked (sensitivity 25-50%): Trachea common radiographic “blind spot”
Lungs usually normal, even when trachea nearly occluded
Patterns
Intraluminal (40%)
Apex to base tumor ratio > 1
Margin usually smooth
Wall-thickening (50%)
Apex to base tumor ratio < 1
Spindle-shaped
Margin usually smooth
Exophytic (10%)
Mediastinal widening
DIFFERENTIAL DIAGNOSIS
Wegener Granulomatosis
Vasculitis triad: Sinus, lung, renal disease
Cavitary nodules
Subglottic stenosis
Does not spare posterior tracheal membrane
Amyloidosis
Tracheobronchial most common form of amyloidosis
Nodular or diffuse deposits in airway wall, when diffuse involves entire wall
30% calcify
Does not spare posterior tracheal membrane
Laryngotracheal Papillomatosis
Human papilloma virus
Multiple solid or cystic pulmonary nodules
At risk to develop squamous cell carcinoma (2%)
Does not spare posterior tracheal membrane
Tracheopathia Osteochondroplastica
Enchondrosis of cartilaginous rings
Usually small, do not compromise tracheal lumen
Spares posterior tracheal membrane
Relapsing Polychondritis
Autoimmune disorder destroys cartilage (airway, ear, nose)
Spares posterior tracheal membrane
PATHOLOGY
General Features
General path comments: Normal components of tracheal wall include C-shaped cartilage rings, muscle, columnar epithelium, lymphoid tissue, mucus glands
Etiology
Top 5 (90% of tracheal tumors): Squamous cell carcinoma, adenoid cystic carcinoma, carcinoid, squamous cell papilloma, mucoepidermoid carcinoma
Squamous cell papilloma most common benign tumor
Squamous cell carcinoma (33%)
Smoking-related
Adenoid cystic carcinoma (33%)
Not associated with cigarette smoking
Neuroendocrine tumors
Carcinoid
Small cell carcinoma
Salivary gland tumors
Myoepithelioma
Oncocytoma
Mucoepidermoid carcinoma
Mesenchymal tumors
Fibroma
Hemangioma
Paraganglioma
Glomus tumorRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



